Department of Medicine (Austin Health), The University of Melbourne, Melbourne, Victoria 3084, Australia.
Department of Endocrinology, Austin Health, Heidelberg, Victoria 3084, Australia.
J Clin Endocrinol Metab. 2023 Aug 18;108(9):e871-e884. doi: 10.1210/clinem/dgad180.
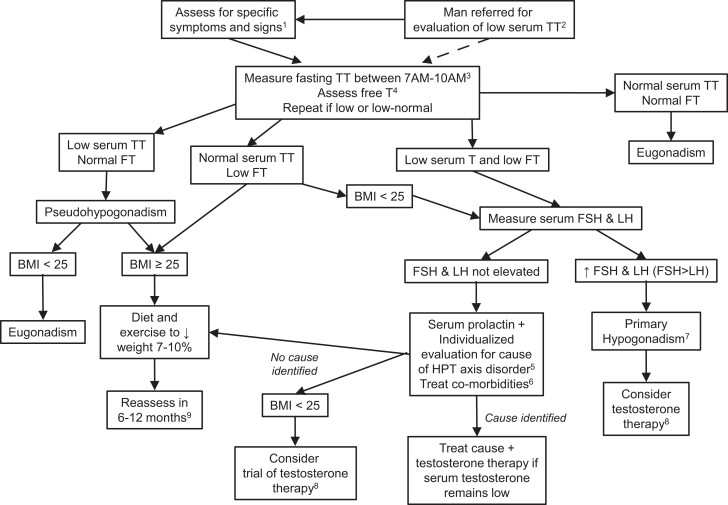
Although testosterone replacement in men with classic hypogonadism due to an identified pathology of the hypothalamic-pituitary-testicular axis is uncontroversial, the role of testosterone treatment for men with age-related declines in circulating testosterone is unclear. This is due to the lack of large, long-term testosterone therapy trials assessing definitive clinical endpoints. However, men ≥50 years of age, particularly those who have a body mass index >25 kg/m2 and multiple comorbidities, commonly present with clinical features of androgen deficiency and low serum testosterone concentrations. Clinicians are faced with the question whether to initiate testosterone therapy, a difficult dilemma that entails a benefit-risk analysis with limited evidence from clinical trials. Using a case scenario, we present a practical approach to the clinical assessment and management of such men.
尽管对于由于下丘脑-垂体-睾丸轴的明确病理导致的经典性腺功能减退症的男性,进行睾丸激素替代治疗是无争议的,但对于因年龄相关的循环睾丸激素水平下降而接受睾丸激素治疗的男性,其作用尚不清楚。这是由于缺乏评估明确临床终点的大型、长期睾丸激素治疗试验。然而,年龄≥50 岁的男性,特别是那些体重指数(BMI)>25 kg/m2 且合并多种疾病的男性,通常会出现雄激素缺乏和血清睾丸激素浓度低的临床特征。临床医生面临的问题是是否开始睾丸激素治疗,这是一个涉及获益-风险分析的难题,其证据有限来自临床试验。我们使用案例情景,提出了一种实用的方法来对这些男性进行临床评估和管理。