Department of Public Health, Sapporo Medical University School of Medicine, S-1, W-17, Chuo-Ku, Sapporo, 060-8556, Japan.
Department of Pediatrics, Sapporo Medical University School of Medicine, Sapporo, Japan.
Int J Health Geogr. 2023 Mar 30;22(1):7. doi: 10.1186/s12942-023-00328-5.
Prehospital delay in reaching a percutaneous coronary intervention (PCI) facility is a major problem preventing early coronary reperfusion in patients with ST-elevation myocardial infarction (STEMI). The aim of this study was to identify modifiable factors that contribute to the interval from symptom onset to arrival at a PCI-capable center with a focus on geographical infrastructure-dependent and -independent factors.
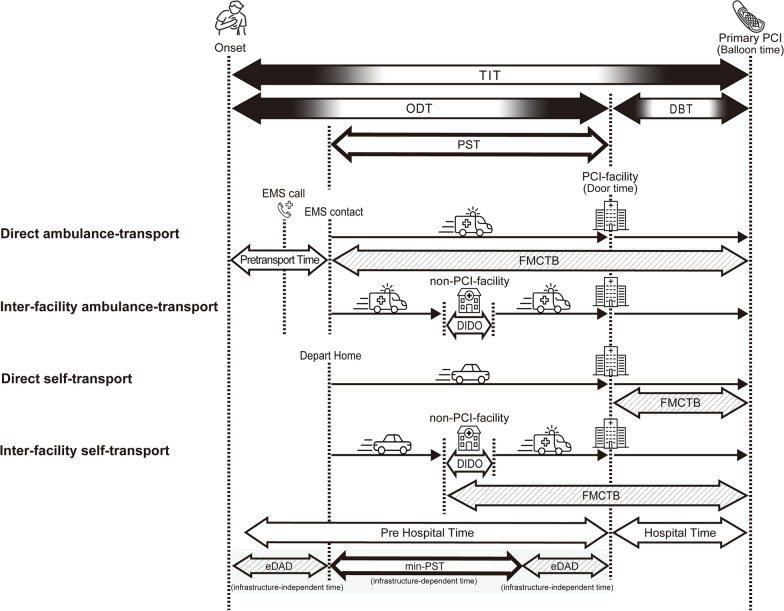
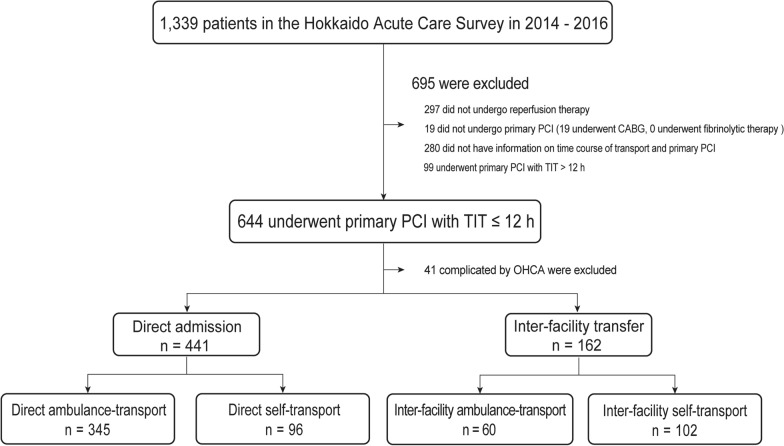
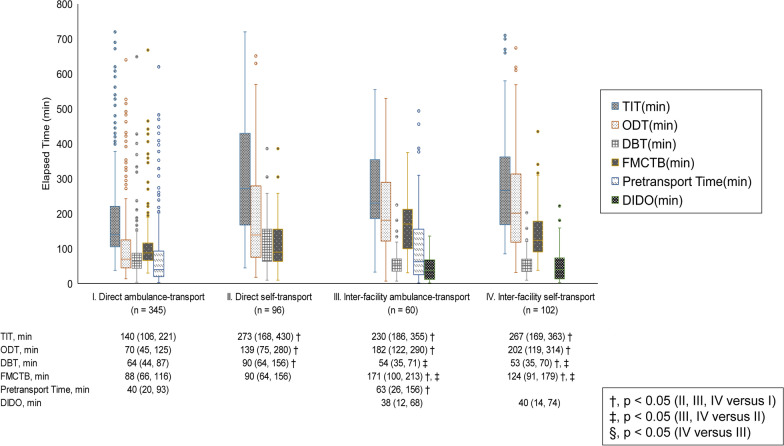
We analyzed data from 603 STEMI patients who received primary PCI within 12 h of symptom onset in the Hokkaido Acute Coronary Care Survey. We defined onset-to-door time (ODT) as the interval from the onset of symptoms to arrival at the PCI facility and we defined door-to-balloon time (DBT) as the interval from arrival at the PCI facility to PCI. We analyzed the characteristics and factors of each time interval by type of transportation to PCI facilities. In addition, we used geographical information system software to calculate the minimum prehospital system time (min-PST), which represents the time required to reach a PCI facility based on geographical factors. We then subtracted min-PST from ODT to find the estimated delay-in-arrival-to-door (eDAD), which represents the time required to reach a PCI facility independent of geographical factors. We investigated the factors related to the prolongation of eDAD.
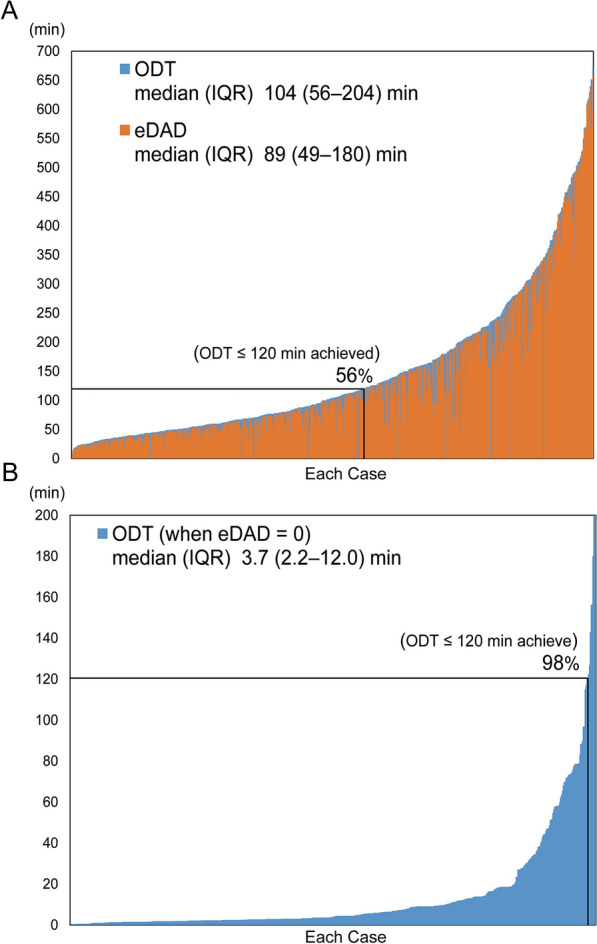
DBT (median [IQR]: 63 [44, 90] min) was shorter than ODT (median [IQR]: 104 [56, 204] min) regardless of the type of transportation. However, ODT was more than 120 min in 44% of the patients. The min-PST (median [IQR]: 3.7 [2.2, 12.0] min) varied widely among patients, with a maximum of 156 min. Prolongation of eDAD (median [IQR]: 89.1 [49, 180] min) was associated with older age, absence of a witness, onset at night, no emergency medical services (EMS) call, and transfer via a non-PCI facility. If eDAD was zero, ODT was projected to be less than 120 min in more than 90% of the patients.
The contribution of geographical infrastructure-dependent time in prehospital delay was substantially smaller than that of geographical infrastructure-independent time. Intervention to shorten eDAD by focusing on factors such as older age, absence of a witness, onset at night, no EMS call, and transfer via a non-PCI facility appears to be an important strategy for reducing ODT in STEMI patients. Additionally, eDAD may be useful for evaluating the quality of STEMI patient transport in areas with different geographical conditions.
在到达经皮冠状动脉介入治疗(PCI)机构之前的院前延迟是阻止 ST 段抬高型心肌梗死(STEMI)患者早期冠状动脉再灌注的主要问题。本研究的目的是确定导致从症状发作到到达具有 PCI 能力的中心的时间间隔的可改变因素,重点是地理基础设施依赖和独立的因素。
我们分析了北海道急性冠状动脉护理调查中 603 例在症状发作后 12 小时内接受直接 PCI 的 STEMI 患者的数据。我们将从症状发作到到达 PCI 设施的时间定义为就诊至门时间(ODT),将从到达 PCI 设施到 PCI 的时间定义为门至球囊时间(DBT)。我们根据前往 PCI 设施的交通方式分析了每个时间间隔的特征和因素。此外,我们使用地理信息系统软件计算最小的院前系统时间(min-PST),它代表基于地理因素到达 PCI 设施所需的时间。然后,我们从 ODT 中减去 min-PST 以找到到达 PCI 设施的估计延迟时间(eDAD),它代表独立于地理因素到达 PCI 设施所需的时间。我们研究了与 eDAD 延长相关的因素。
无论交通方式如何,DBT(中位数[IQR]:63 [44, 90] 分钟)均短于 ODT(中位数[IQR]:104 [56, 204] 分钟)。然而,44%的患者的 ODT 超过 120 分钟。患者之间的 min-PST(中位数[IQR]:3.7 [2.2, 12.0] 分钟)差异很大,最大为 156 分钟。eDAD 延长(中位数[IQR]:89.1 [49, 180] 分钟)与年龄较大、无目击者、夜间发作、无紧急医疗服务(EMS)呼叫以及通过非 PCI 设施转移有关。如果 eDAD 为零,则超过 90%的患者的 ODT 预计将小于 120 分钟。
在院前延迟中,地理基础设施依赖时间的贡献明显小于地理基础设施独立时间的贡献。通过关注年龄较大、无目击者、夜间发作、无 EMS 呼叫以及通过非 PCI 设施转移等因素来缩短 eDAD 的干预措施似乎是减少 STEMI 患者 ODT 的重要策略。此外,eDAD 可能有助于评估具有不同地理条件的 STEMI 患者转运的质量。