Kenya Medical Research Institute, Centre for Global Health Research, Kisumu, Kenya.
Kenya Medical Research Institute-Wellcome Trust Research Programme, Kilifi, Kenya.
BMC Med. 2023 Mar 31;21(1):122. doi: 10.1186/s12916-023-02787-w.
Respiratory syncytial virus (RSV) is among the leading childhood causes of viral pneumonia worldwide. Establishing RSV-associated morbidity and mortality is important in informing the development, delivery strategies, and evaluation of interventions.
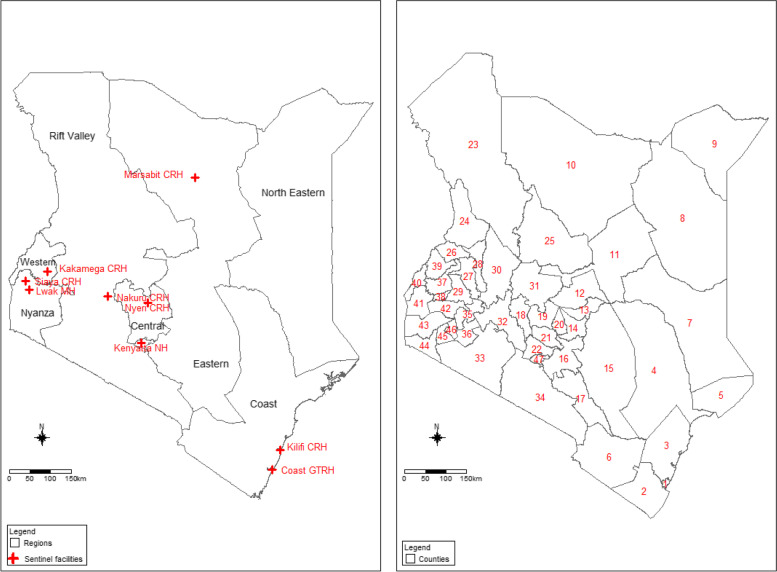
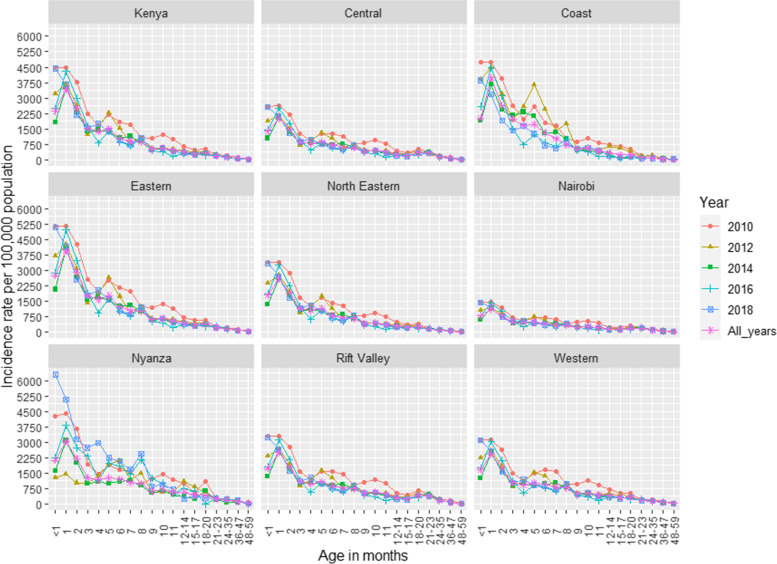
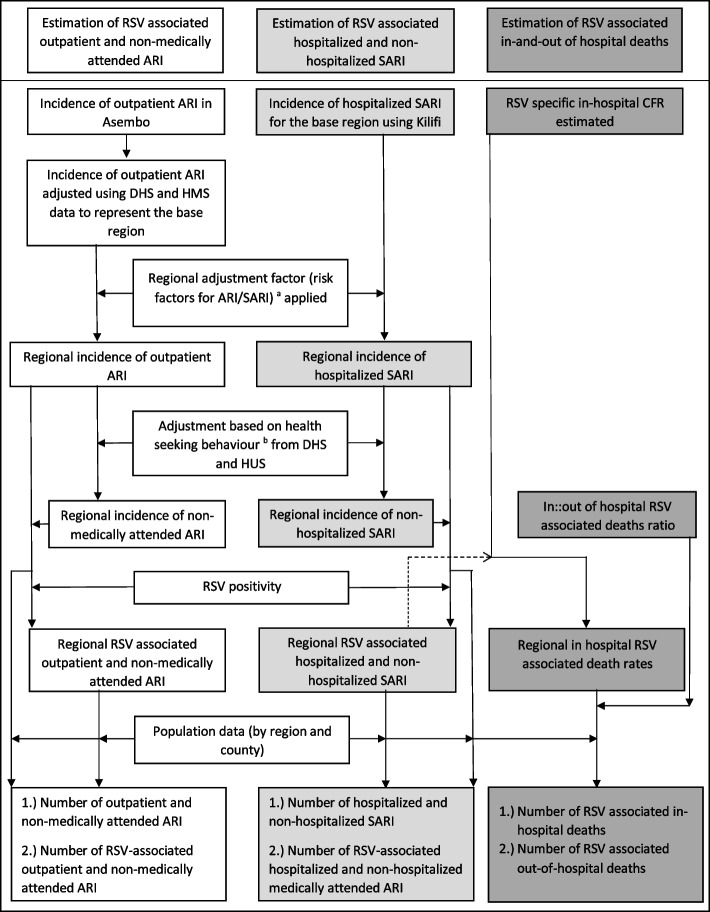
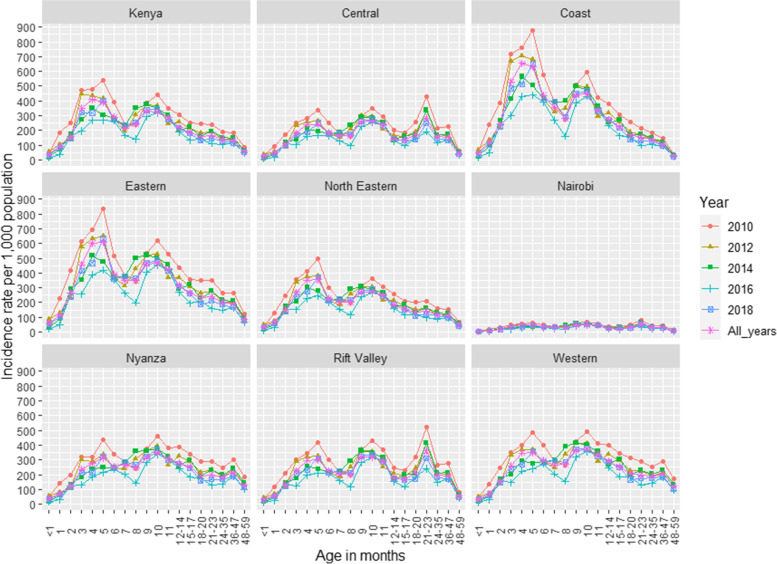
Using data collected during 2010-2018 from base regions (population-based surveillance studies in western Kenya and the Kilifi Health and Demographic Surveillance Study), we estimated age-specific rates of acute respiratory illness (ARI), severe acute respiratory illness (SARI-defined as hospitalization with cough or difficulty breathing with onset within the past 10 days), and SARI-associated deaths. We extrapolated the rates from the base regions to other regions of Kenya, while adjusting for risk factors of ARI and healthcare seeking behavior, and finally applied the proportions of RSV-positive cases identified from various sentinel and study facilities to the rates to obtain regional age-specific rates of RSV-associated outpatient and non-medically attended ARI and hospitalized SARI and severe ARI that was not hospitalized (non-hospitalized SARI). We applied age-specific RSV case fatality ratios to SARI to obtain estimates of RSV-associated in- and out-of-hospital deaths.
Among Kenyan children aged < 5 years, the estimated annual incidence of outpatient and non-medically attended RSV-associated ARI was 206 (95% credible interval, CI; 186-229) and 226 (95% CI; 204-252) per 1000 children, respectively. The estimated annual rates of hospitalized and non-hospitalized RSV-associated SARI were 349 (95% CI; 303-404) and 1077 (95% CI; 934-1247) per 100,000 children respectively. The estimated annual number of in- and out-of-hospital deaths associated with RSV infection in Kenya were 539 (95% CI; 420-779) and 1921 (95% CI; 1495-2774), respectively. Children aged < 6 months had the highest burden of RSV-associated severe disease: 2075 (95% CI; 1818-2394) and 44 (95% CI 25-71) cases per 100,000 children for hospitalized SARI and in-hospital deaths, respectively.
Our findings suggest a substantial disease burden due to RSV infection, particularly among younger children. Prioritizing development and use of maternal vaccines and affordable long-lasting monoclonal antibodies could help reduce this burden.
呼吸道合胞病毒(RSV)是全球导致儿童病毒性肺炎的主要病原体之一。确定 RSV 相关发病率和死亡率对于制定、实施和评估干预措施非常重要。
我们利用 2010 年至 2018 年期间从基础区域(肯尼亚西部的基于人群的监测研究和基利菲健康和人口监测研究)收集的数据,估计了急性呼吸道疾病(ARI)、严重急性呼吸道疾病(SARI-定义为在过去 10 天内因咳嗽或呼吸困难住院的病例)和 SARI 相关死亡的年龄特异性发病率。我们根据 ARI 的危险因素和医疗服务利用情况对基础区域的发病率进行了调整,最后将从各种哨点和研究机构确定的 RSV 阳性病例比例应用于这些发病率,以获得肯尼亚其他地区的年龄特异性 RSV 相关门诊和非医疗就诊 ARI 以及住院 SARI 和未住院的严重 SARI(非住院 SARI)的发病率。我们将年龄特异性 RSV 病死率应用于 SARI,以获得 RSV 相关住院和非住院死亡的估计值。
在肯尼亚 5 岁以下儿童中,估计门诊和非医疗就诊的 RSV 相关 ARI 的年发病率分别为每 1000 名儿童 206 例(95%可信区间,CI;186-229)和 226 例(95% CI;204-252)。住院和非住院的 RSV 相关 SARI 的年发病率分别为每 100,000 名儿童 349 例(95% CI;303-404)和 1077 例(95% CI;934-1247)。肯尼亚因 RSV 感染导致的住院和非住院相关死亡的年估计数分别为 539 例(95% CI;420-779)和 1921 例(95% CI;1495-2774)。年龄<6 个月的儿童 RSV 相关严重疾病负担最高:每 100,000 名儿童中分别有 2075 例(95% CI;1818-2394)和 44 例(95% CI 25-71)住院 SARI 和院内死亡病例。
我们的研究结果表明,RSV 感染导致了相当大的疾病负担,尤其是在年幼的儿童中。优先开发和使用母源性疫苗和负担得起的长效单克隆抗体可能有助于减轻这一负担。