Department for Infectious Disease Epidemiology, London School of Hygiene & Tropical Medicine, London, UK.
Centre for Mathematical Modelling of Infectious Diseases, London School of Hygiene & Tropical Medicine, London, UK.
BMC Med. 2023 Mar 31;21(1):120. doi: 10.1186/s12916-023-02806-w.
Respiratory syncytial virus (RSV) causes a substantial burden of acute lower respiratory infection in children under 5 years, particularly in low- and middle-income countries (LMICs). Maternal vaccine (MV) and next-generation monoclonal antibody (mAb) candidates have been shown to reduce RSV disease in infants in phase 3 clinical trials. The cost-effectiveness of these biologics has been estimated using disease burden data from global meta-analyses, but these are sensitive to the detailed age breakdown of paediatric RSV disease, for which there have previously been limited data.
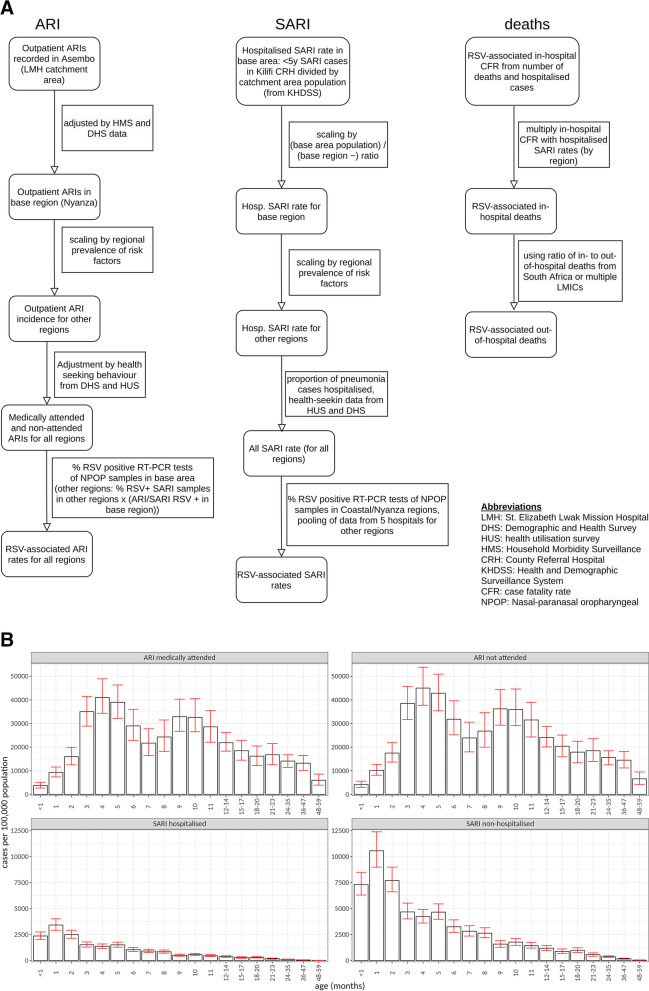
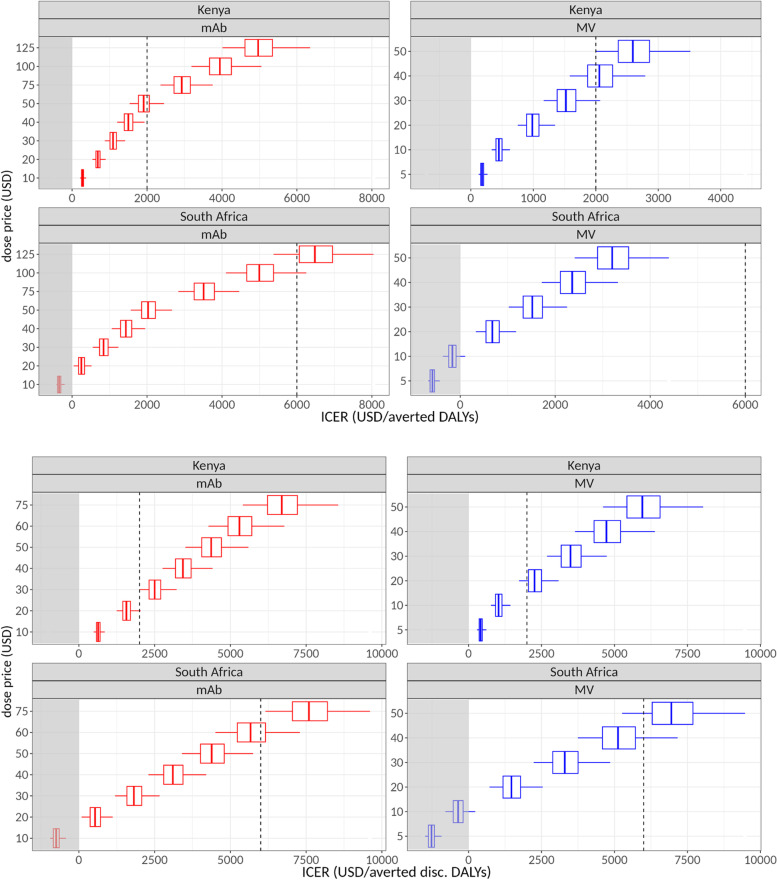
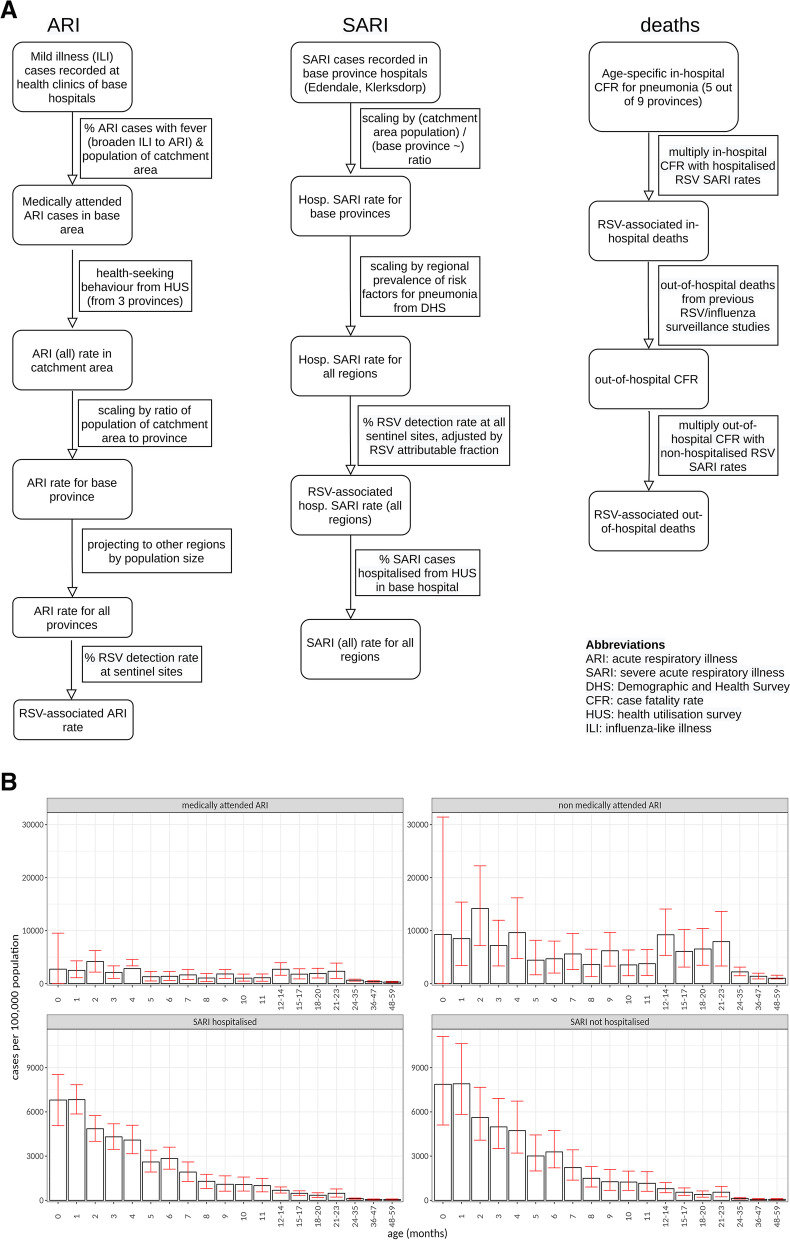
We use original hospital-based incidence data from South Africa (ZAF) and Kenya (KEN) collected between 2010 and 2018 of RSV-associated acute respiratory infection (ARI), influenza-like illness (ILI), and severe acute respiratory infection (SARI) as well as deaths with monthly age-stratification, supplemented with data on healthcare-seeking behaviour and costs to the healthcare system and households. We estimated the incremental cost per DALY averted (incremental cost-effectiveness ratio or ICER) of public health interventions by MV or mAb for a plausible range of prices (5-50 USD for MV, 10-125 USD for mAb), using an adjusted version of a previously published health economic model of RSV immunisation.
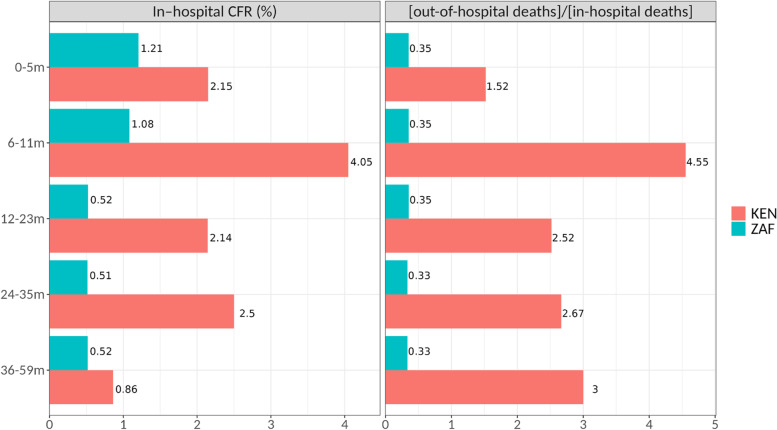
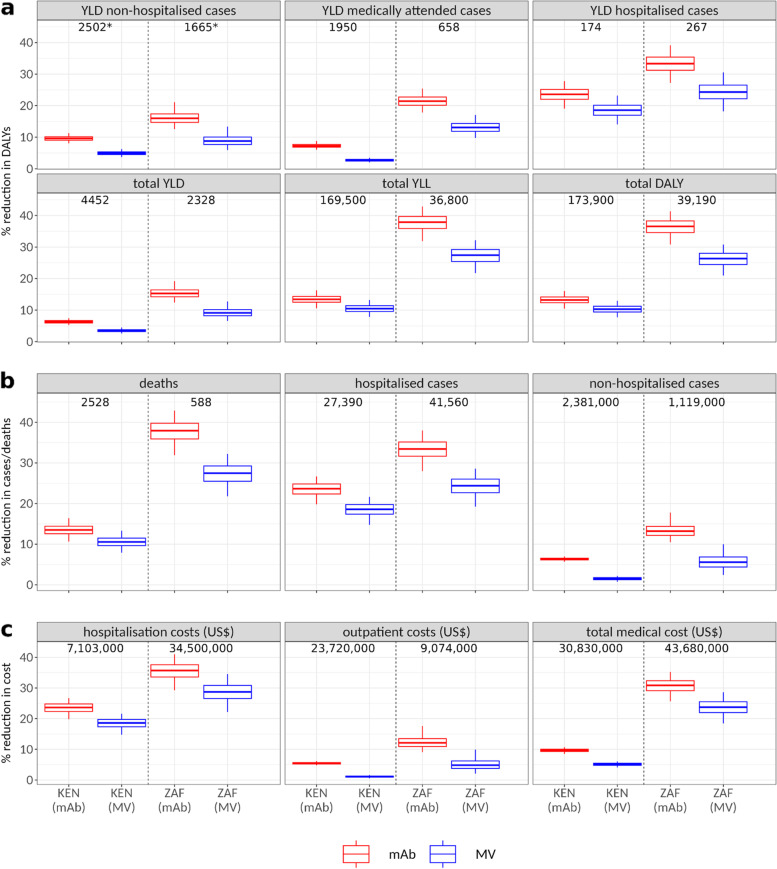
Our data show higher disease incidence for infants younger than 6 months of age in the case of Kenya and South Africa than suggested by earlier projections from community incidence-based meta-analyses of LMIC data. Since MV and mAb provide protection for these youngest age groups, this leads to a substantially larger reduction of disease burden and, therefore, more favourable cost-effectiveness of both interventions in both countries. Using the latest efficacy data and inferred coverage levels based on antenatal care (ANC-3) coverage (KEN: 61.7%, ZAF: 75.2%), our median estimate of the reduction in RSV-associated deaths in children under 5 years in Kenya is 10.5% (95% CI: 7.9, 13.3) for MV and 13.5% (10.7, 16.4) for mAb, while in South Africa, it is 27.4% (21.6, 32.3) and 37.9% (32.3, 43.0), respectively. Starting from a dose price of 5 USD, in Kenya, net cost (for the healthcare system) per (undiscounted) DALY averted for MV is 179 (126, 267) USD, rising to 1512 (1166, 2070) USD at 30 USD per dose; for mAb, it is 684 (543, 895) USD at 20 USD per dose and 1496 (1203, 1934) USD at 40 USD per dose. In South Africa, a MV at 5 USD per dose would be net cost-saving for the healthcare system and net cost per DALY averted is still below the ZAF's GDP per capita at 40 USD dose price (median: 2350, 95% CI: 1720, 3346). For mAb in ZAF, net cost per DALY averted is 247 (46, 510) USD at 20 USD per dose, rising to 2028 (1565, 2638) USD at 50 USD per dose and to 6481 (5364, 7959) USD at 125 USD per dose.
Incorporation of new data indicating the disease burden is highly concentrated in the first 6 months of life in two African settings suggests that interventions against RSV disease may be more cost-effective than previously estimated.
呼吸道合胞病毒(RSV)在 5 岁以下儿童中引起大量急性下呼吸道感染,特别是在中低收入国家(LMICs)。已证明母体疫苗(MV)和下一代单克隆抗体(mAb)候选药物可降低婴儿在 3 期临床试验中的 RSV 疾病。使用来自全球荟萃分析的疾病负担数据估计了这些生物制剂的成本效益,但这些数据对儿科 RSV 疾病的详细年龄分布很敏感,而此前对此类数据的了解有限。
我们使用南非(ZAF)和肯尼亚(KEN)的原始基于医院的发病率数据,这些数据是在 2010 年至 2018 年期间收集的,包括 RSV 相关的急性呼吸道感染(ARI)、流感样疾病(ILI)和严重急性呼吸道感染(SARI)以及与每月年龄分层相关的死亡病例,并补充了有关医疗保健寻求行为以及对医疗保健系统和家庭的成本的数据。我们使用以前发表的 RSV 免疫健康经济模型的调整版本,估计了 MV 或 mAb 进行公共卫生干预的增量成本效益(每避免一个 DALY 的增量成本效益比或 ICER),价格范围为 5-50 美元(MV),10-125 美元(mAb)。
我们的数据显示,肯尼亚和南非的婴儿年龄小于 6 个月的疾病发病率高于之前社区发病率基于 LMIC 数据的荟萃分析的预测。由于 MV 和 mAb 为这些最年轻的年龄组提供了保护,因此这大大降低了疾病负担,因此这两种干预措施在这两个国家的成本效益都更加有利。使用最新的疗效数据和基于产前护理(ANC-3)覆盖率的推断覆盖率(KEN:61.7%,ZAF:75.2%),我们对肯尼亚 5 岁以下儿童与 RSV 相关的死亡人数减少的中位数估计为 10.5%(95%CI:7.9,13.3),MV 为 13.5%(10.7,16.4),mAb 为 13.5%(10.7,16.4)。在南非,分别为 27.4%(21.6,32.3)和 37.9%(32.3,43.0)。从 5 美元的剂量价格开始,在肯尼亚,MV 每(未贴现)避免一个 DALY 的净成本(对医疗保健系统而言)为 179 美元(126 美元,267 美元),上升至 30 美元/剂量时为 1512 美元(1166 美元,2070 美元);对于 mAb,每剂量 20 美元为 684 美元(543 美元,895 美元),每剂量 40 美元为 1496 美元(1203 美元,1934 美元)。在南非,MV 的 5 美元剂量对医疗保健系统来说是净成本节约,并且每避免一个 DALY 的净成本仍然低于 ZAF 的人均 GDP(中位数:2350 美元,95%CI:1720 美元,3346 美元)。对于 ZAF 的 mAb,每剂量 20 美元的净成本为每避免一个 DALY 的 247 美元(46 美元,510 美元),上升至每剂量 50 美元的 2028 美元(1565 美元,2638 美元)和每剂量 125 美元的 6481 美元(5364 美元,7959 美元)。
纳入新数据表明疾病负担高度集中在两个非洲国家的生命的头 6 个月表明,针对 RSV 疾病的干预措施可能比以前估计的更具成本效益。