Department of Medicine, University Health Network, University of Toronto, Toronto, ON, Canada.
Genetics and Genome Biology Program, The Hospital for Sick Children, Toronto, ON, Canada.
Front Endocrinol (Lausanne). 2023 Mar 17;14:1146099. doi: 10.3389/fendo.2023.1146099. eCollection 2023.
Insulin resistance (IR) with associated compensatory hyperinsulinemia (HI) are early abnormalities in the etiology of prediabetes (preT2D) and type 2 diabetes (T2D). IR and HI also associate with increased erythrocytosis. Hemoglobin A1c (HbA1c) is commonly used to diagnose and monitor preT2D and T2D, but can be influenced by erythrocytosis independent of glycemia.
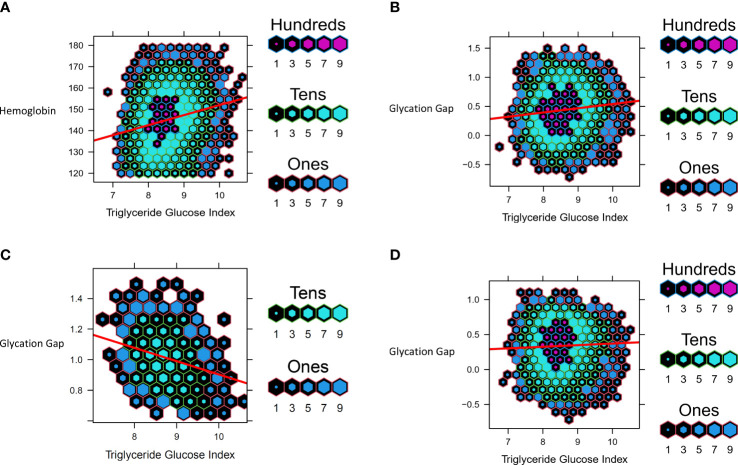
We undertook bidirectional Mendelian randomization (MR) in individuals of European ancestry to investigate potential causal associations between increased fasting insulin adjusted for BMI (FI), erythrocytosis and its non-glycemic impact on HbA1c. We investigated the association between the triglyceride-glucose index (TGI), a surrogate measure of IR and HI, and glycation gap (difference between measured HbA1c and predicted HbA1c derived from linear regression of fasting glucose) in people with normoglycemia and preT2D.
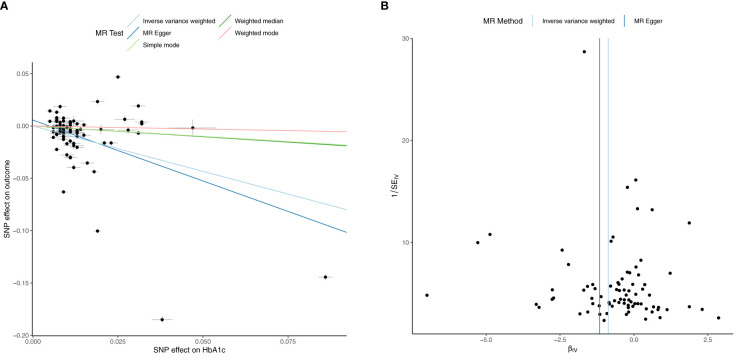
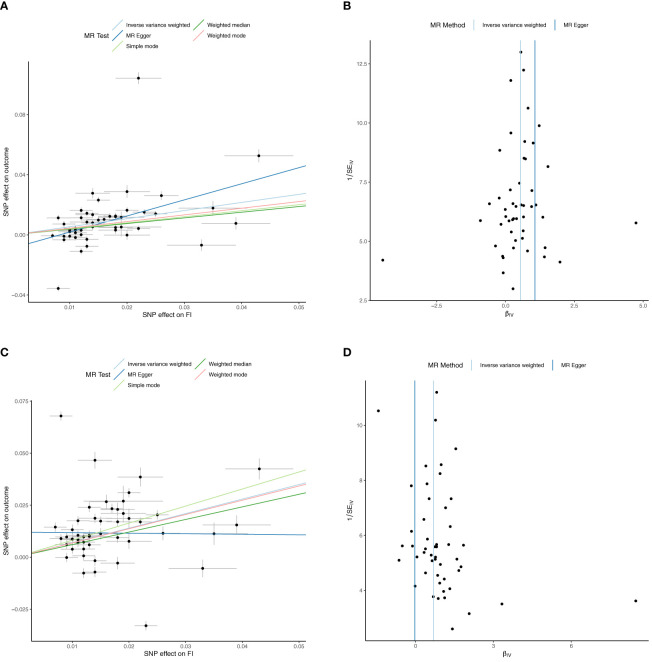
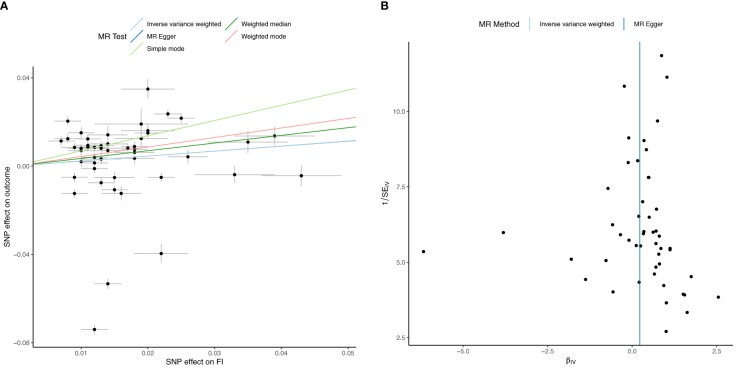
Inverse variance weighted MR (IVWMR) suggested that increased FI increases hemoglobin (Hb, b=0.54 ± 0.09, p=2.7 x 10), red cell count (RCC, b=0.54 ± 0.12, p=5.38x10) and reticulocyte (RETIC, b=0.70 ± 0.15, p=2.18x10). Multivariable MR indicated that increased FI did not impact HbA1c (b=0.23 ± 0.16, p=0.162) but reduced HbA1c after adjustment for T2D (b=0.31 ± 0.13, p=0.016). Increased Hb (b=0.03 ± 0.01, p=0.02), RCC (b=0.02 ± 0.01, p=0.04) and RETIC (b=0.03 ± 0.01, p=0.002) might modestly increase FI. In the observational cohort, increased TGI associated with decreased glycation gap, (i.e., measured HbA1c was lower than expected based on fasting glucose, (b=-0.09 ± 0.009, p<0.0001)) in people with preT2D but not in those with normoglycemia (b=0.02 ± 0.007, p<0.0001).
MR suggests increased FI increases erythrocytosis and might potentially decrease HbA1c by non-glycemic effects. Increased TGI, a surrogate measure of increased FI, associates with lower-than-expected HbA1c in people with preT2D. These findings merit confirmatory studies to evaluate their clinical significance.
胰岛素抵抗(IR)伴代偿性高胰岛素血症(HI)是前驱糖尿病(preT2D)和 2 型糖尿病(T2D)发病机制中的早期异常。IR 和 HI 也与红细胞增多症有关。糖化血红蛋白(HbA1c)常用于诊断和监测 preT2D 和 T2D,但不受血糖影响的红细胞增多症会影响其结果。
我们在欧洲血统个体中进行了双向孟德尔随机化(MR),以研究空腹胰岛素(FI)、红细胞增多症及其对 HbA1c 的非血糖影响与增加之间的潜在因果关联。我们调查了在血糖正常和前驱糖尿病患者中,甘油三酯-葡萄糖指数(TGI)与糖化间隙(由空腹葡萄糖线性回归得出的实测 HbA1c 与预测 HbA1c 之间的差异)之间的关系。
逆方差加权 MR(IVWMR)表明,FI 增加会增加血红蛋白(Hb,b=0.54±0.09,p=2.7x10)、红细胞计数(RCC,b=0.54±0.12,p=5.38x10)和网织红细胞(RETIC,b=0.70±0.15,p=2.18x10)。多变量 MR 表明,FI 增加不会影响 HbA1c(b=0.23±0.16,p=0.162),但调整 T2D 后会降低 HbA1c(b=0.31±0.13,p=0.016)。Hb 适度增加(b=0.03±0.01,p=0.02)、RCC(b=0.02±0.01,p=0.04)和 RETIC(b=0.03±0.01,p=0.002)可能会增加 FI。在观察性队列中,TGI 增加与糖化间隙减小相关,(即实测 HbA1c 低于基于空腹葡萄糖的预期值,(b=-0.09±0.009,p<0.0001)),在前驱糖尿病患者中,但在血糖正常的患者中则不然(b=0.02±0.007,p<0.0001)。
MR 表明,FI 增加会增加红细胞增多症,并且可能通过非血糖作用降低 HbA1c。前驱糖尿病患者中,代表 FI 增加的 TGI 增加与低于预期的 HbA1c 相关。这些发现值得进一步的验证性研究来评估其临床意义。