Neurology, Boston Medical Center, Boston, USA.
Radiology, Boston Medical Center, Boston, USA.
Clin Neuroradiol. 2023 Sep;33(3):801-811. doi: 10.1007/s00062-023-01284-0. Epub 2023 Apr 3.
The proper imaging modality for use in the selection of patients for endovascular thrombectomy (EVT) presenting in the late window remains controversial, despite current guidelines advocating the use of advanced imaging in this population. We sought to understand if clinicians with different specialty training differ in their approach to patient selection for EVT in the late time window.
We conducted an international survey of stroke and neurointerventional clinicians between January and May 2022 with questions focusing on imaging and treatment decisions of large vessel occlusion (LVO) patients presenting in the late window. Interventional neurologists, interventional neuroradiologists, and endovascular neurosurgeons were defined as interventionists whereas all other specialties were defined as non-interventionists. The non-interventionist group was defined by all other specialties of the respondents: stroke neurologist, neuroradiologist, emergency medicine physician, trainee (fellows and residents) and others.
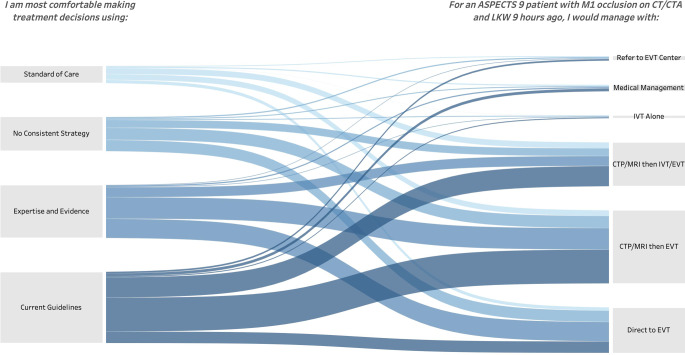
Of 3000 invited to participate, 1506 (1027 non-interventionists, 478 interventionists, 1 declined to specify) physicians completed the study. Interventionist respondents were more likely to proceed directly to EVT (39.5% vs. 19.5%; p < 0.0001) compared to non-interventionist respondents in patients with favorable ASPECTS (Alberta Stroke Program Early CT Score). Despite no difference in access to advanced imaging, interventionists were more likely to prefer CT/CTA alone (34.8% vs. 21.0%) and less likely to prefer CT/CTA/CTP (39.1% vs. 52.4%) for patient selection (p < 0.0001). When faced with uncertainty, non-interventionists were more likely to follow clinical guidelines (45.1% vs. 30.2%) while interventionists were more likely to follow their assessment of evidence (38.7% vs. 27.0%) (p < 0.0001).
Interventionists were less likely to use advanced imaging techniques in selecting LVO patients presenting in the late window and more likely to base their decisions on their assessment of evidence rather than published guidelines. These results reflect gaps between interventionists and non-interventionists reliance on clinical guidelines, the limits of available evidence, and clinician belief in the utility of advanced imaging.
尽管目前的指南主张在该人群中使用先进的影像学检查,但对于在晚期时间窗内进行血管内血栓切除术 (EVT) 的患者,选择合适的影像学检查方法仍存在争议。我们旨在了解具有不同专业培训的临床医生在晚期时间窗内对 EVT 患者选择方面的方法是否存在差异。
我们于 2022 年 1 月至 5 月期间对中风和神经介入临床医生进行了一项国际调查,调查内容主要集中在大血管闭塞 (LVO) 患者在晚期出现时的影像学和治疗决策。介入神经科医生、介入神经放射科医生和血管神经外科医生被定义为介入医生,而所有其他专业被定义为非介入医生。非介入医生组由受访者的所有其他专业组成:中风神经科医生、神经放射科医生、急诊医生、受训者(研究员和住院医师)和其他人员。
在邀请的 3000 名参与者中,有 1506 名(1027 名非介入医生、478 名介入医生、1 名拒绝具体说明)医生完成了研究。与非介入医生相比,介入医生更倾向于直接进行 EVT(39.5%对 19.5%;p<0.0001),在 ASPECTS 评分良好的患者中(Alberta Stroke Program Early CT Score)。尽管在获得先进影像学检查方面没有差异,但介入医生更倾向于单独使用 CT/CTA(34.8%对 21.0%),而不太倾向于使用 CT/CTA/CTP(39.1%对 52.4%)进行患者选择(p<0.0001)。当面临不确定性时,非介入医生更倾向于遵循临床指南(45.1%对 30.2%),而介入医生更倾向于遵循他们对证据的评估(38.7%对 27.0%)(p<0.0001)。
介入医生在选择晚期出现 LVO 的患者时不太倾向于使用先进的影像学技术,而更倾向于根据自己对证据的评估做出决策,而不是遵循已发表的指南。这些结果反映了介入医生和非介入医生对临床指南的依赖程度、现有证据的局限性以及临床医生对先进影像学技术的效用的信念之间的差距。