Luo Leilei, Zhou Guanen, Meng Fanlei, Liu Shuling, Wang Sifei, Dou Yuchao, Lu Da, Wei Ming
Department of Neurology, Tianjin Huanhu Hospital, Tianjin, China.
Department of Neurosurgery, The Second Hospital of Tianjin Medical University, Tianjin, China.
Front Neurol. 2024 Jul 25;15:1400524. doi: 10.3389/fneur.2024.1400524. eCollection 2024.
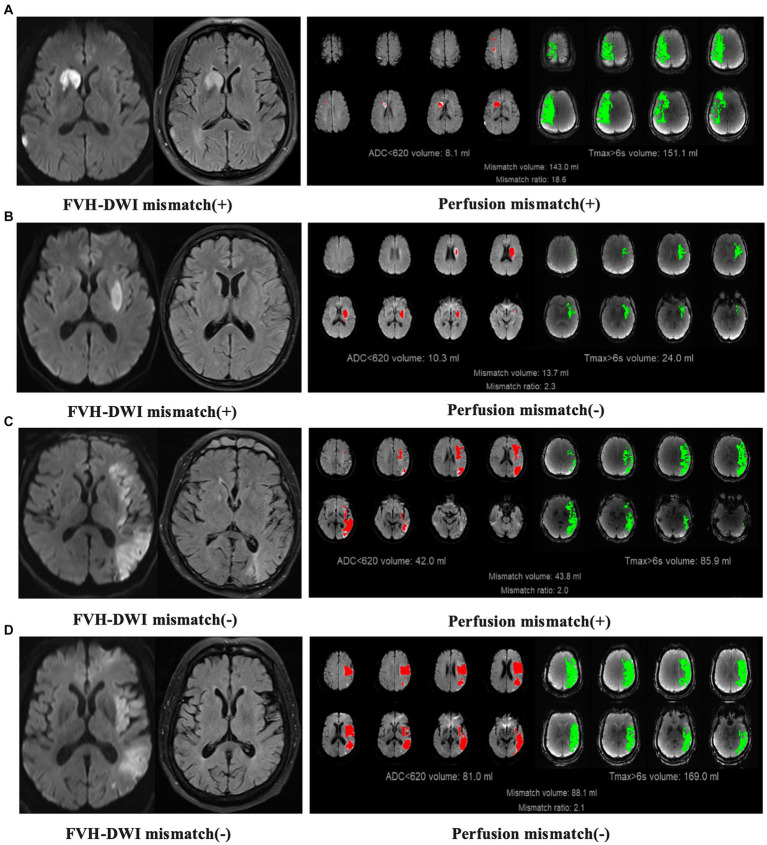
The clinical impact of patient selection using FLAIR vascular hyperintensity (FVH)-diffusion-weighted imaging (DWI) mismatch for endovascular thrombectomy (EVT) in patients who have been symptomatic for over 6 h remains unclear. Herein, a retrospective study was conducted to compare the inter-rater reliability and clinical outcomes of patients selected for thrombectomy based on FVH-DWI mismatch with perfusion.
Patients with anterior-circulation large-vessel occlusion selected simultaneously with MRI and perfusion imaging in the late time window from a single-center retrospective study were categorized into EVT-applicable (FVH-DWI mismatch on MRI or perfusion imaging meeting the DEFUSE3 standards) and EVT-inapplicable groups based on MRI and perfusion imaging. The primary outcome was the 90-day functional independence rate. Safety outcomes encompassed symptomatic intracranial hemorrhage and mortality in 90 days. We assessed the consistency of the two profiles and compared the differences in functional independence rates of EVT patients among the EVT-applicable groups determined by MRI and perfusion.
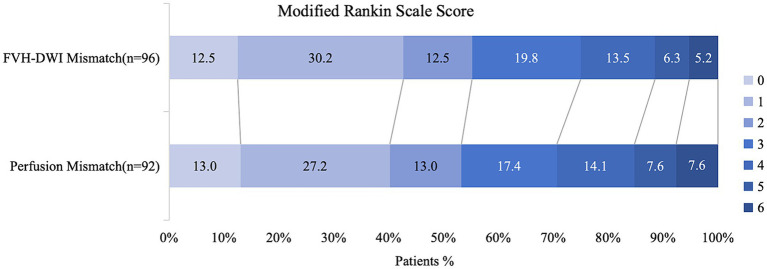
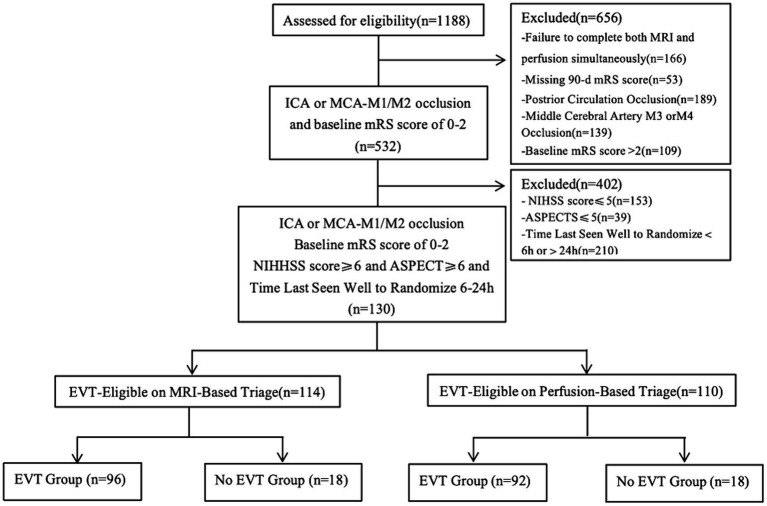
A total of 130 patients were enrolled, of which 114 were classified into the EVT-applicable group after triaging using MRI images. In this group, 96 patients underwent EVT, with 53 of them (55.2%) achieving functional independence. A total of 110 patients were divided into EVT-applicable group based on perfusion, among which 92 underwent EVT, with 49 of them (53.2%) achieving functional independence. The consistency of identifying EVT indication was moderate between two groups (κ = 0.42, 95% CI, 0.17-0.67). The functional independence rate was comparable between patients in the two EVT-applicable groups based on the two methods (55.2% vs. 53.2%, = 0.789).
MRI triaging based on FVH-DWI mismatch showed moderate inter-rater reliability compared with perfusion-based triage and comparable efficacy in predicting clinical outcomes after EVT.
对于症状出现超过6小时的患者,使用液体衰减反转恢复序列血管高信号(FVH)-弥散加权成像(DWI)不匹配来选择血管内血栓切除术(EVT)的临床影响尚不清楚。在此,进行了一项回顾性研究,以比较基于FVH-DWI不匹配与灌注选择进行血栓切除术的患者的评分者间可靠性和临床结局。
在一项单中心回顾性研究的晚期时间窗中,同时进行MRI和灌注成像选择的前循环大血管闭塞患者,根据MRI和灌注成像分为EVT适用组(MRI或灌注成像上的FVH-DWI不匹配符合DEFUSE3标准)和EVT不适用组。主要结局是90天功能独立率。安全性结局包括症状性颅内出血和90天内死亡率。我们评估了两种评估的一致性,并比较了由MRI和灌注确定的EVT适用组中EVT患者功能独立率的差异。
共纳入130例患者,其中114例在使用MRI图像进行分诊后被分类为EVT适用组。在该组中,96例患者接受了EVT,其中53例(55.2%)实现了功能独立。共有110例患者根据灌注被分为EVT适用组,其中92例接受了EVT,其中49例(53.2%)实现了功能独立。两组之间识别EVT适应证的一致性为中等(κ = 0.42, 95% CI, 0.17 - 0.67)。基于两种方法的两个EVT适用组患者的功能独立率相当(55.2%对53.2%,P = 0.789)。
与基于灌注的分诊相比,基于FVH-DWI不匹配的MRI分诊显示出中等的评分者间可靠性,并且在预测EVT后的临床结局方面疗效相当。