Department of Neurology, Columbia University Irving Medical Center, New York, New York, USA.
Department of Neurology, Hospital of the University of Pennsylvania, Philadelphia, Pennsylvania, USA.
Epilepsia. 2023 Jun;64(6):1568-1581. doi: 10.1111/epi.17602. Epub 2023 Apr 24.
Stereotactic laser amygdalohippocampotomy (SLAH) is an appealing option for patients with temporal lobe epilepsy, who often require intracranial monitoring to confirm mesial temporal seizure onset. However, given limited spatial sampling, it is possible that stereotactic electroencephalography (stereo-EEG) may miss seizure onset elsewhere. We hypothesized that stereo-EEG seizure onset patterns (SOPs) may differentiate between primary onset and secondary spread and predict postoperative seizure control. In this study, we characterized the 2-year outcomes of patients who underwent single-fiber SLAH after stereo-EEG and evaluated whether stereo-EEG SOPs predict postoperative seizure freedom.
This retrospective five-center study included patients with or without mesial temporal sclerosis (MTS) who underwent stereo-EEG followed by single-fiber SLAH between August 2014 and January 2022. Patients with causative hippocampal lesions apart from MTS or for whom the SLAH was considered palliative were excluded. An SOP catalogue was developed based on literature review. The dominant pattern for each patient was used for survival analysis. The primary outcome was 2-year Engel I classification or recurrent seizures before then, stratified by SOP category.
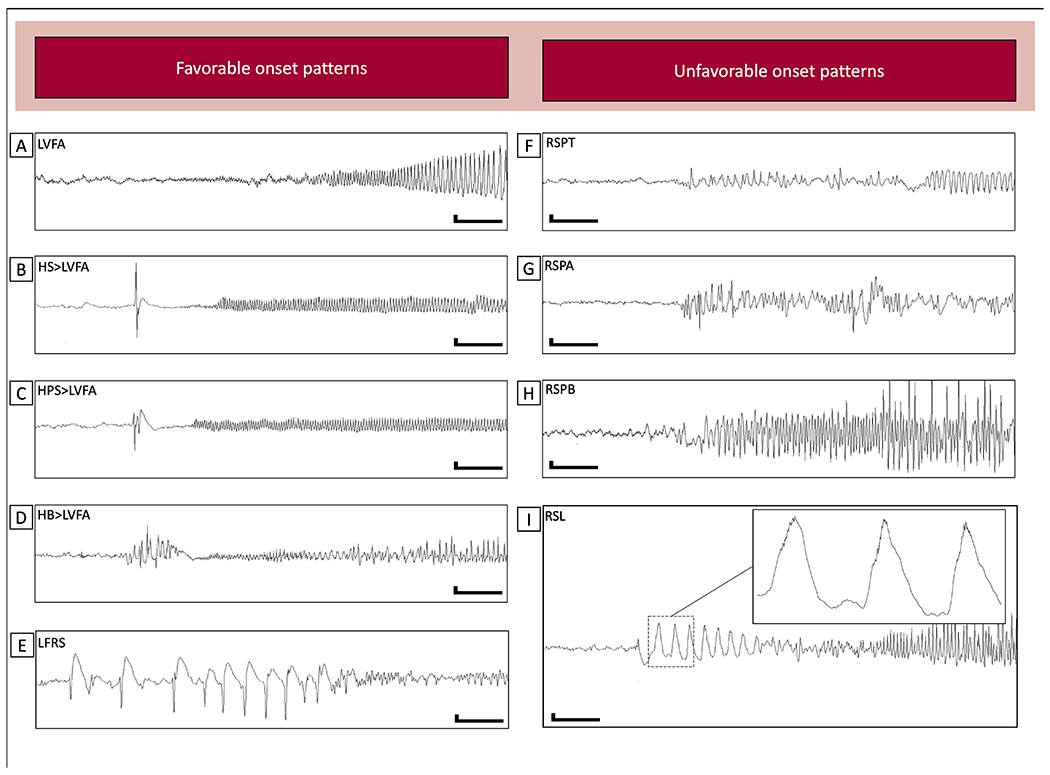
Fifty-eight patients were included, with a mean follow-up duration of 39 ± 12 months after SLAH. Overall 1-, 2-, and 3-year Engel I seizure freedom probability was 54%, 36%, and 33%, respectively. Patients with SOPs, including low-voltage fast activity or low-frequency repetitive spiking, had a 46% 2-year seizure freedom probability, compared to 0% for patients with alpha or theta frequency repetitive spiking or theta or delta frequency rhythmic slowing (log-rank test, p = .00015).
Patients who underwent SLAH after stereo-EEG had a low probability of seizure freedom at 2 years, but SOPs successfully predicted seizure recurrence in a subset of patients. This study provides proof of concept that SOPs distinguish between hippocampal seizure onset and spread and supports using SOPs to improve selection of SLAH candidates.
立体定向激光杏仁核海马切开术(SLAH)是颞叶癫痫患者的一种有吸引力的选择,他们通常需要颅内监测来确认内侧颞叶发作起始。然而,由于空间采样有限,立体定向脑电图(stereo-EEG)可能会错过其他部位的发作起始。我们假设 stereo-EEG 发作起始模式(SOP)可以区分原发性发作和继发性扩散,并预测术后癫痫控制。在这项研究中,我们描述了在 stereo-EEG 后接受单纤维 SLAH 的患者的 2 年结果,并评估了 stereo-EEG SOP 是否可以预测术后无癫痫发作。
这是一项回顾性的五中心研究,纳入了 2014 年 8 月至 2022 年 1 月期间在接受 stereo-EEG 后行单纤维 SLAH 的患者,无论有无内侧颞叶硬化(MTS)。排除了除 MTS 之外还有海马病变的病因或认为 SLAH 是姑息性的患者。根据文献综述开发了 SOP 目录。每个患者的主导模式用于生存分析。主要结果是根据 SOP 类别,以 2 年 Engel I 分类或在此之前的复发性癫痫来分层。
共纳入 58 例患者,SLAH 后平均随访时间为 39±12 个月。总体而言,1、2 和 3 年的 Engel I 癫痫无发作率分别为 54%、36%和 33%。SOP 包括低电压快活动或低频重复尖波的患者,2 年癫痫无发作率为 46%,而α或θ频率重复尖波或θ或δ频率节律性减慢的患者为 0%(对数秩检验,p=0.00015)。
接受 stereo-EEG 后行 SLAH 的患者 2 年无癫痫发作的可能性较低,但 SOP 成功地预测了一部分患者的癫痫复发。这项研究提供了概念验证,即 SOP 可区分海马的发作起始和扩散,并支持使用 SOP 来改善 SLAH 候选者的选择。