Jaber Samir, De Jong Audrey, Schaefer Maximilian S, Zhang Jiaqiang, Ma Xiaowen, Hao Xinrui, Zhou Shujing, Lv Shang, Banner-Goodspeed Valerie, Niu Xiuhua, Sfara Thomas, Talmor Daniel
Anesthesiology and Intensive Care; Anesthesia and Critical Care Department B, Saint Eloi Teaching Hospital, PhyMedExp, University of Montpellier, INSERM U1046, 1; 80 avenue Augustin Fliche, Montpellier cedex 5, Montpellier, France.
Centre Hospitalier Universitaire Montpellier, 34295, Montpellier, France.
Ann Intensive Care. 2023 Apr 4;13(1):26. doi: 10.1186/s13613-023-01124-x.
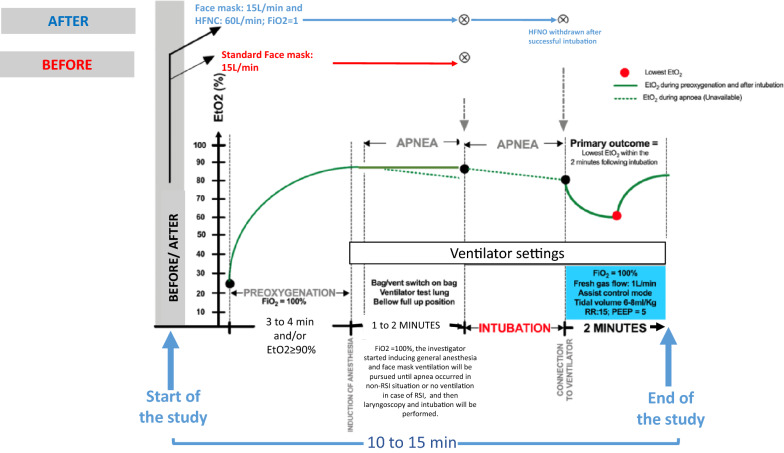
Combining oxygen facemask with apnoeic oxygenation using high-flow-nasal-oxygen (HFNO) for preoxygenation in the operating room has not been studied against standard oxygen facemask alone. We hypothesized that facemask-alone would be associated with lower levels of lowest end-tidal oxygen (EtO2) within 2 min after intubation in comparison with facemask combined with HFNO.
In an international prospective before-after multicentre study, we included adult patients intubated in the operating room from September 2022 to December 2022. In the before period, preoxygenation was performed with facemask-alone, which was removed during laryngoscopy. In the after period, facemask combined with HFNO was used for preoxygenation and HFNO for apnoeic oxygenation during laryngoscopy. HFNO was maintained throughout intubation. The primary outcome was the lowest EtO2 within 2 min after intubation. The secondary outcome was SpO2 ≤ 95% within 2 min after intubation. Subgroup analyses were performed in patients without and with obesity. This study was registered 10 August 2022 with ClinicalTrials.gov, number NCT05495841.
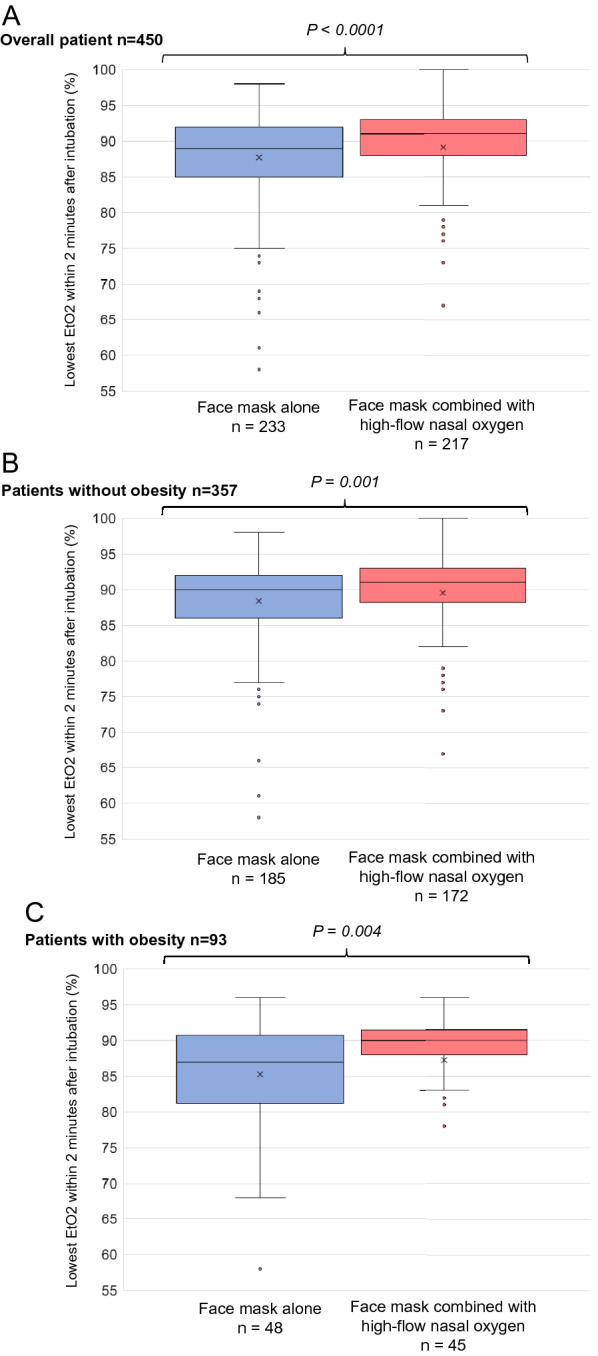
A total of 450 intubations were evaluated, 233 with facemask-alone and 217 with facemask combined with HFNO. In all patients, the lowest EtO2 within 2 min after intubation was significantly lower with facemask-alone than with facemask combined with HFNO, 89 (85-92)% vs 91 (88-93)%, respectively (mean difference - 2.20(- 3.21 to - 1.18), p < 0.001). In patients with obesity, similar results were found [87(82-91)% vs 90(88-92)%, p = 0.004]; as in patients without obesity [90(86-92)% vs 91(89-93)%, p = 0.001)]. SpO2 ≤ 95% was more frequent with facemask-alone (14/232, 6%) than with facemask combined with HFNO (2/215, 1%, p = 0.004). No severe adverse events were recorded.
Combining facemask with HFNO for preoxygenation and apnoeic oxygenation was associated with increased levels of lowest EtO2 within 2 min after intubation and less desaturation.
在手术室中,将氧气面罩与使用高流量鼻氧(HFNO)进行的窒息氧合相结合用于预充氧,尚未与单独使用标准氧气面罩进行对比研究。我们假设,与氧气面罩联合HFNO相比,单独使用氧气面罩在插管后2分钟内的最低呼气末氧(EtO2)水平会更低。
在一项国际前瞻性前后对照多中心研究中,我们纳入了2022年9月至2022年12月在手术室接受插管的成年患者。在前期,单独使用氧气面罩进行预充氧,在喉镜检查时移除。在后期,使用氧气面罩联合HFNO进行预充氧,并在喉镜检查期间使用HFNO进行窒息氧合。在整个插管过程中维持HFNO。主要结局是插管后2分钟内的最低EtO2。次要结局是插管后2分钟内SpO2≤95%。对非肥胖和肥胖患者进行了亚组分析。本研究于2022年8月10日在ClinicalTrials.gov注册,编号为NCT05495841。
共评估了450例插管,其中233例单独使用氧气面罩,217例使用氧气面罩联合HFNO。在所有患者中,单独使用氧气面罩时插管后2分钟内的最低EtO2显著低于氧气面罩联合HFNO时,分别为89(85 - 92)%和91(88 - 93)%(平均差异 - 2.20(- 3.21至 - 1.18),p < 0.001)。在肥胖患者中也发现了类似结果[87(82 - 91)%对90(88 - 92)%,p = 0.004];非肥胖患者中也是如此[90(86 - 92)%对91(89 - 93)%,p = 0.001]。单独使用氧气面罩时SpO2≤95%的情况比氧气面罩联合HFNO时更常见(14/232,6%对2/215,1%,p = 0.004)。未记录到严重不良事件。
将氧气面罩与HFNO联合用于预充氧和窒息氧合,与插管后2分钟内最低EtO2水平升高及去饱和减少相关。