The Advanced Care Research Centre, Usher Institute of Population Health Sciences and Informatics, University of Edinburgh, Edinburgh, United Kingdom.
The Usher Institute of Population Health Sciences and Informatics, University of Edinburgh, Edinburgh, United Kingdom.
PLoS Med. 2023 Apr 4;20(4):e1004208. doi: 10.1371/journal.pmed.1004208. eCollection 2023 Apr.
Multimorbidity prevalence rates vary considerably depending on the conditions considered in the morbidity count, but there is no standardised approach to the number or selection of conditions to include.
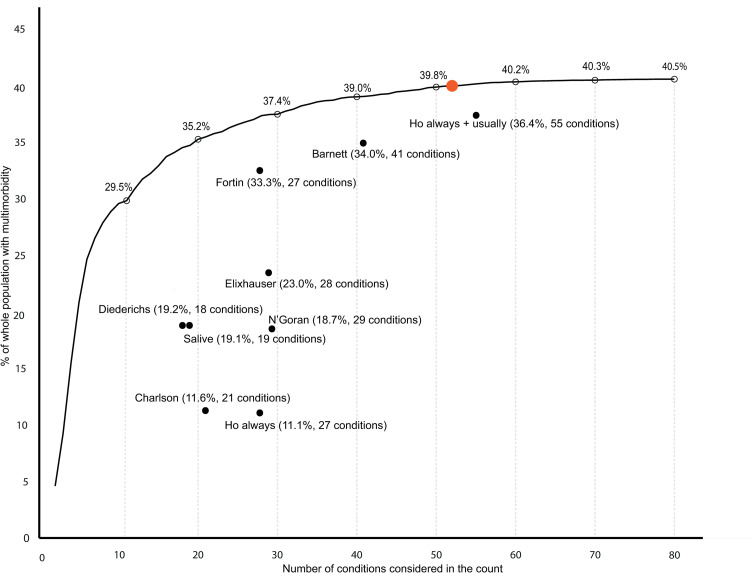
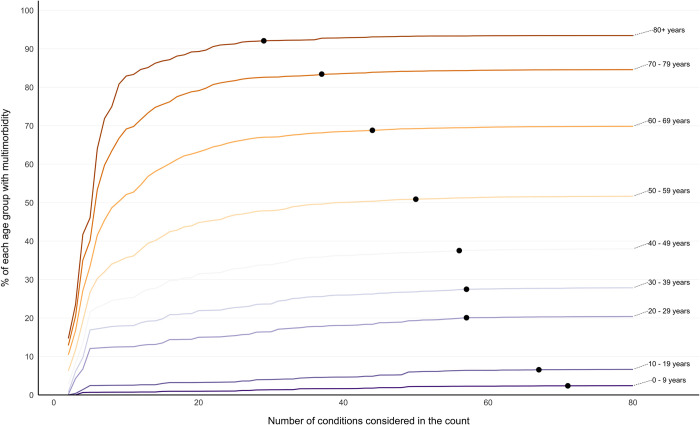
We conducted a cross-sectional study using English primary care data for 1,168,260 participants who were all people alive and permanently registered with 149 included general practices. Outcome measures of the study were prevalence estimates of multimorbidity (defined as ≥2 conditions) when varying the number and selection of conditions considered for 80 conditions. Included conditions featured in ≥1 of the 9 published lists of conditions examined in the study and/or phenotyping algorithms in the Health Data Research UK (HDR-UK) Phenotype Library. First, multimorbidity prevalence was calculated when considering the individually most common 2 conditions, 3 conditions, etc., up to 80 conditions. Second, prevalence was calculated using 9 condition-lists from published studies. Analyses were stratified by dependent variables age, socioeconomic position, and sex. Prevalence when only the 2 commonest conditions were considered was 4.6% (95% CI [4.6, 4.6] p < 0.001), rising to 29.5% (95% CI [29.5, 29.6] p < 0.001) considering the 10 commonest, 35.2% (95% CI [35.1, 35.3] p < 0.001) considering the 20 commonest, and 40.5% (95% CI [40.4, 40.6] p < 0.001) when considering all 80 conditions. The threshold number of conditions at which multimorbidity prevalence was >99% of that measured when considering all 80 conditions was 52 for the whole population but was lower in older people (29 in >80 years) and higher in younger people (71 in 0- to 9-year-olds). Nine published condition-lists were examined; these were either recommended for measuring multimorbidity, used in previous highly cited studies of multimorbidity prevalence, or widely applied measures of "comorbidity." Multimorbidity prevalence using these lists varied from 11.1% to 36.4%. A limitation of the study is that conditions were not always replicated using the same ascertainment rules as previous studies to improve comparability across condition-lists, but this highlights further variability in prevalence estimates across studies.
In this study, we observed that varying the number and selection of conditions results in very large differences in multimorbidity prevalence, and different numbers of conditions are needed to reach ceiling rates of multimorbidity prevalence in certain groups of people. These findings imply that there is a need for a standardised approach to defining multimorbidity, and to facilitate this, researchers can use existing condition-lists associated with highest multimorbidity prevalence.
多种疾病的患病率差异很大,具体取决于发病率计数中考虑的条件,但目前还没有一种标准化的方法来确定纳入的条件数量或选择。
我们使用英国初级保健数据进行了一项横断面研究,共纳入了 1168260 名参与者,他们均为在世并永久注册在 149 家参与普通实践中的人群。本研究的结局指标是当考虑 80 种疾病时,不同数量和选择疾病的情况下,多种疾病(定义为≥2 种疾病)的患病率估计。纳入的疾病特征是在研究中检查的 9 个已发表的疾病清单中的≥1 个,或在英国健康数据研究(HDR-UK)表型库中的表型算法。首先,当考虑最常见的 2 种、3 种等疾病时,计算多种疾病的患病率,最多可达 80 种疾病。其次,使用来自已发表研究的 9 种疾病清单来计算患病率。分析根据依赖变量年龄、社会经济地位和性别进行分层。仅考虑最常见的 2 种疾病时,患病率为 4.6%(95%CI[4.6,4.6],p<0.001),当考虑最常见的 10 种疾病时,患病率为 29.5%(95%CI[29.5,29.6],p<0.001),当考虑最常见的 20 种疾病时,患病率为 35.2%(95%CI[35.1,35.3],p<0.001),当考虑所有 80 种疾病时,患病率为 40.5%(95%CI[40.4,40.6],p<0.001)。当患病率为考虑所有 80 种疾病时的 99%以上时,所需的疾病数量阈值为 52,但在老年人(>80 岁的人群中为 29)中较低,在年轻人(0-9 岁人群中为 71)中较高。我们研究了 9 个已发表的疾病清单;这些清单要么是为测量多种疾病而推荐的,要么是之前研究多种疾病患病率的高引用研究中使用的,要么是广泛应用的“合并症”测量方法。使用这些清单的多种疾病的患病率从 11.1%到 36.4%不等。本研究的一个局限性是,在提高各疾病清单之间的可比性时,并非总是使用相同的确定规则来重复这些疾病,但是这进一步突出了各研究之间的患病率估计值存在差异。
在本研究中,我们观察到,不同数量和选择疾病会导致多种疾病的患病率存在很大差异,并且在某些人群中达到多种疾病患病率的上限需要不同数量的疾病。这些发现表明,需要一种标准化的方法来定义多种疾病,为了促进这一点,研究人员可以使用与最高多种疾病患病率相关的现有疾病清单。