Ramai Daryl, McEntire Dan M, Tavakolian Kameron, Heaton Joseph, Chandan Saurabh, Dhindsa Banreet, Dhaliwal Amaninder, Maida Marcello, Anderloni Andrea, Facciorusso Antonio, Adler Douglas G
Gastroenterology & Hepatology, University of Utah Health, Salt Lake City, Utah, United States.
Department of Medicine, Jersey Shore University Medical Center, Neptune City, New Jersey, United States.
Endosc Int Open. 2023 Apr 4;11(4):E330-E339. doi: 10.1055/a-1994-6214. eCollection 2023 Apr.
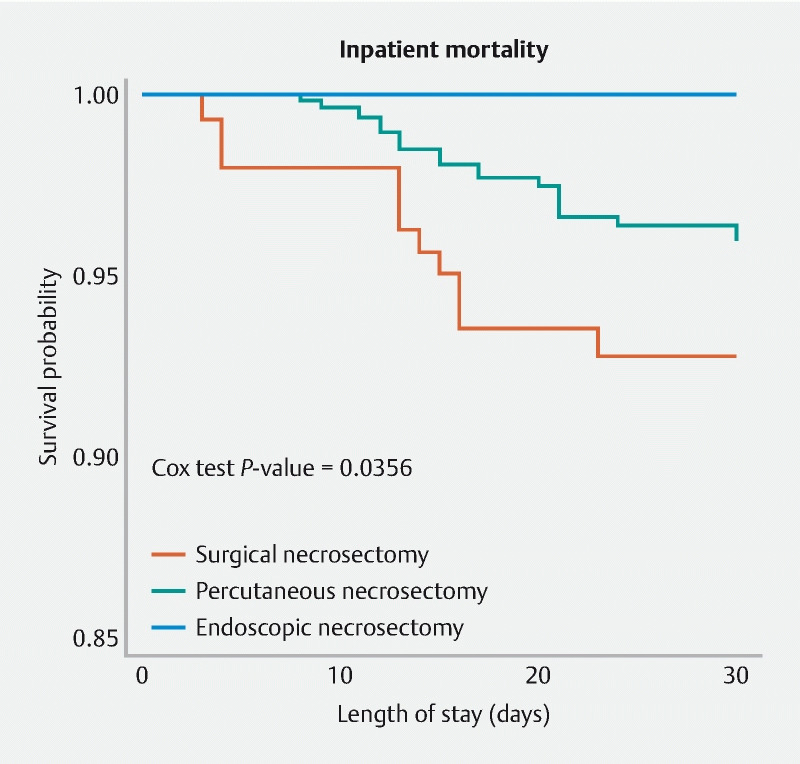
Pancreatic necrosis is an independent predictor of morbidity and mortality among patients with acute pancreatitis. We compared the safety and outcomes of three techniques including endoscopic necrosectomy, fluoroscopy-guided percutaneous necrosectomy by an interventional radiologist, and surgical necrosectomy. Using the Nationwide Readmissions Database, we identified hospitalized patients who underwent pancreatic necrosectomy from 2016 to 2019. They were identified using the International Classification of Diseases, 10th Revision, Procedure Coding System. Of the 2,281 patients meeting the selection criteria, the method of pancreatic necrosectomy was as follows: endoscopy (n = 672), percutaneous (n = 1,338), and surgery (n = 271). Compared to surgery, the rate of mortality was lowest for endoscopy (hazard ratio (HR) 0.27; 95 % CI 0.08-0.90; = 0.033) followed by percutaneous (HR 0.44; 95 % CI, 0.20-0.98; = 0.045). Endoscopy was associated with less post-procedure bleeding compared to percutaneous and surgical necrosectomy ( < 0.001), as well as lower rates of post-procedure renal failure ( < 0.001) and respiratory failure ( = 0.002). Endoscopy was associated with average shorter lengths of stay and total hospital costs when compared with percutaneous and surgical approaches, respectively (20.1 vs 25.8 vs 38.3 days; < 0.001) and ($ 57K vs $ 76K vs $ 123K; < 0.001). Endoscopic necrosectomy is associated with significantly lower risk of inpatient mortality, adverse events, length of stay, and cost when compared to percutaneous and surgical approaches.
胰腺坏死是急性胰腺炎患者发病和死亡的独立预测因素。我们比较了三种技术的安全性和结果,包括内镜坏死组织清除术、由介入放射科医生进行的透视引导下经皮坏死组织清除术和外科坏死组织清除术。利用全国再入院数据库,我们确定了2016年至2019年期间接受胰腺坏死组织清除术的住院患者。他们是使用国际疾病分类第十版手术编码系统确定的。在符合选择标准的2281例患者中,胰腺坏死组织清除术的方法如下:内镜(n = 672)、经皮(n = 1338)和手术(n = 271)。与手术相比,内镜治疗的死亡率最低(风险比(HR)0.27;95%可信区间0.08 - 0.90;P = 0.033),其次是经皮治疗(HR 0.44;95%可信区间0.20 - 0.98;P = 0.045)。与经皮和外科坏死组织清除术相比,内镜治疗术后出血较少(P < 0.001),术后肾衰竭发生率较低(P < 0.001)和呼吸衰竭发生率较低(P = 0.002)。与经皮和手术方法相比,内镜治疗分别与平均住院时间较短和总住院费用较低相关(20.1天对25.8天对38.3天;P < 0.001)和(5.7万美元对7.6万美元对12.3万美元;P < 0.001)。与经皮和手术方法相比,内镜坏死组织清除术与住院死亡率、不良事件、住院时间和费用的风险显著降低相关。