Haug Erik Skaaheim, Myklebust Tor Åge, Juliebø-Jones Patrick, Reisæter Lars Anders Rokne, Aas Kirsti, Berg Arne Stenrud, Müller Christoph, Hofmann Bjørn, Størkersen Øystein, Nilsen Kim L, Johannesen Tom Børge, Beisland Christian
Department of Urology Vestfold Hospital Trust Tønsberg Norway.
Institute of Cancer Genomics and Informatics Oslo University Hospital Oslo Norway.
BJUI Compass. 2023 Jan 10;4(3):331-338. doi: 10.1002/bco2.214. eCollection 2023 May.
The aim of this study is to evaluate the 2015 introduction of prebiopsy magnetic resonance imaging of the prostate (MRI-P) as the standard of care for diagnosing prostate cancer (PCa) by the Norwegian public health care authorities. There were three specific objectives of this study: first, to evaluate the consequences of using different TNM manuals for clinical T-staging (cT-staging) in a national setting; second, to determine if the data reveals that MRI-P based cT-staging is superior to digital rectal examination (DRE)-based cT-staging compared with pathological T-stage (pT-stage) post radical prostatectomy; and third, to assess whether treatment allocations have changed over time.
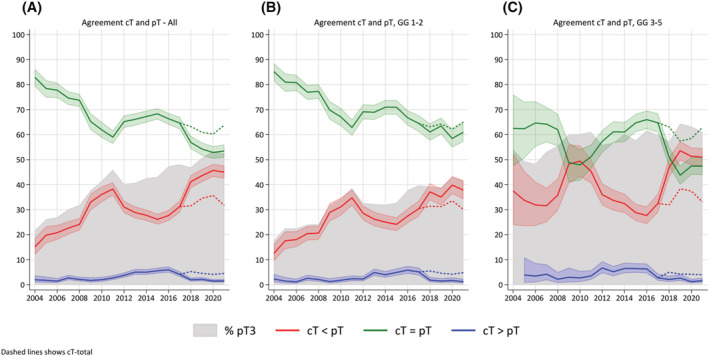
All patients registered in the Norwegian Prostate Cancer Registry between 2004 and 2021 were retrieved and 5538 were eligible for inclusion. Concordance between clinical T-stage (cT-stage) and pT-stage was assessed by percentage agreement, Cohen's kappa and Gwet's agreement.
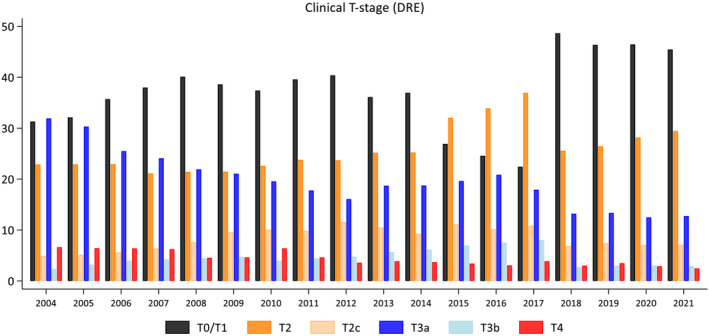
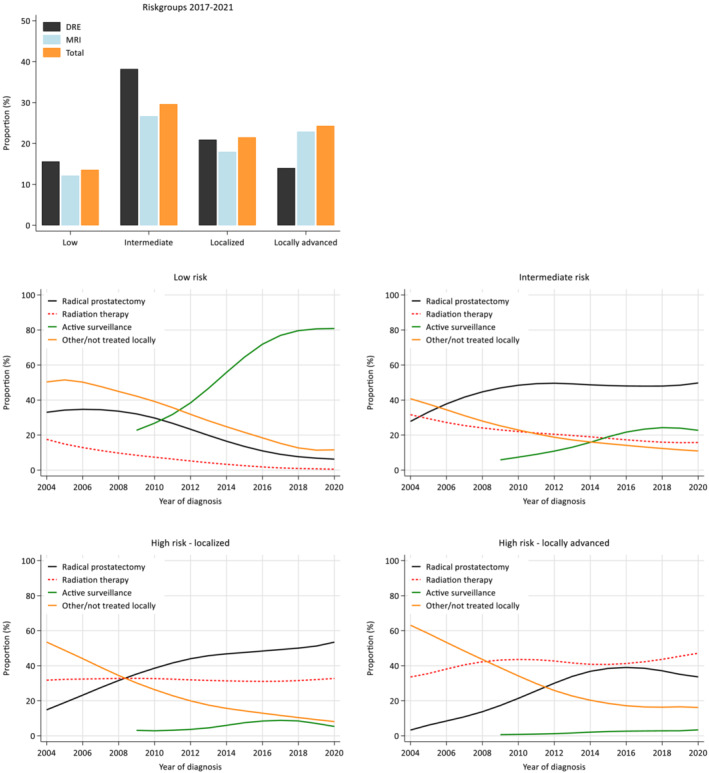
MR visualisation of lesions influences reporting of tumour extension beyond DRE findings. Agreement between cT-stage and pT-stage declined from 2004 to 2009, which coincided with an increase in the percentage being pT3. From 2010, agreement increased, which aligned with changes in cT-staging and the introduction of MRI-P. From 2017, regarding the reporting of cT-DRE and cT-Total (overall cT-stage), agreement diminished for cT-DRE but remained relatively stable (>60%) for cT-Total. Regarding treatment allocation, the study suggests that staging with MRI-P has shifted treatment towards radiotherapy in locally advanced high-risk disease.
Introduction of MRI-P has affected cT-stage reporting. Agreement between cT-stage and pT-stage appears to have improved. This study suggests that use of MRI-P influences treatment decisions in certain patient subgroups.
本研究旨在评估挪威公共卫生保健当局于2015年将前列腺活检前磁共振成像(MRI-P)作为诊断前列腺癌(PCa)的护理标准的情况。本研究有三个具体目标:第一,评估在全国范围内使用不同的TNM手册进行临床T分期(cT分期)的后果;第二,确定数据是否显示基于MRI-P的cT分期与根治性前列腺切除术后的病理T分期(pT分期)相比,优于基于直肠指检(DRE)的cT分期;第三,评估治疗分配是否随时间发生了变化。
检索了2004年至2021年在挪威前列腺癌登记处登记的所有患者,其中5538例符合纳入标准。通过百分比一致性、科恩kappa系数和格韦特一致性评估临床T分期(cT分期)与pT分期之间的一致性。
病变的磁共振成像可视化影响了超出DRE检查结果的肿瘤扩展报告。cT分期与pT分期之间的一致性在2004年至2009年下降,这与pT3比例的增加同时发生。从2010年起,一致性增加,这与cT分期的变化和MRI-P的引入相一致。从2017年起,关于cT-DRE和cT-Total(总体cT分期)的报告,cT-DRE的一致性降低,但cT-Total保持相对稳定(>60%)。关于治疗分配,该研究表明,使用MRI-P已将局部晚期高危疾病的治疗转向放疗。
MRI-P的引入影响了cT分期报告。cT分期与pT分期之间的一致性似乎有所改善。本研究表明,使用MRI-P会影响某些患者亚组的治疗决策。