Department of Neurology, National Neuroscience Institute, Singapore, Singapore.
Duke-NUS Medical School, Singapore, Singapore.
J Neurol. 2023 Jun;270(6):2817-2825. doi: 10.1007/s00415-023-11692-4. Epub 2023 Apr 7.
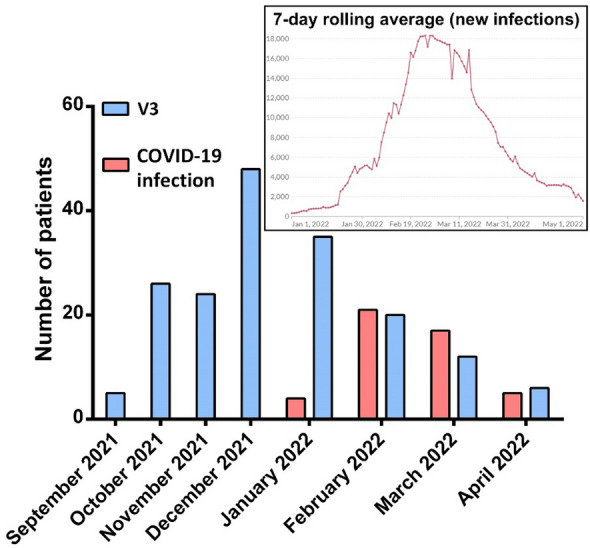
The SARS-CoV-2 Omicron variant appears to cause milder infections, however, its capacity for immune evasion and high transmissibility despite vaccination remains a concern, particularly in immunosuppressed patients. Herein, we investigate the incidence and risk factors for COVID-19 infection in vaccinated adult patients with Multiple Sclerosis (MS), Aquaporin-4-antibody Neuromyelitis Optica Spectrum Disorder (AQP4-Ab NMOSD), and Myelin Oligodendrocyte Glycoprotein-antibody associated disease (MOGAD) during the Omicron subvariant BA.1/2 wave in Singapore.
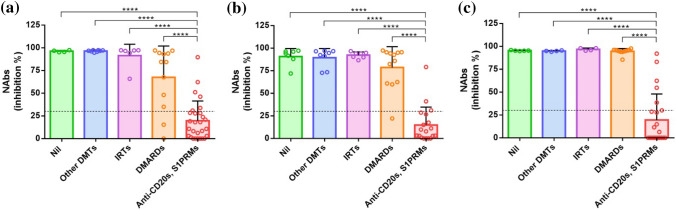
This was a prospective observational study conducted at the National Neuroscience Institute, Singapore. Only patients who had at least two doses of mRNA vaccines were included. Data on demographics, disease characteristics, COVID-19 infections and vaccinations, and immunotherapies were collected. SARS-CoV-2 neutralising antibodies were measured at various time points after vaccination.
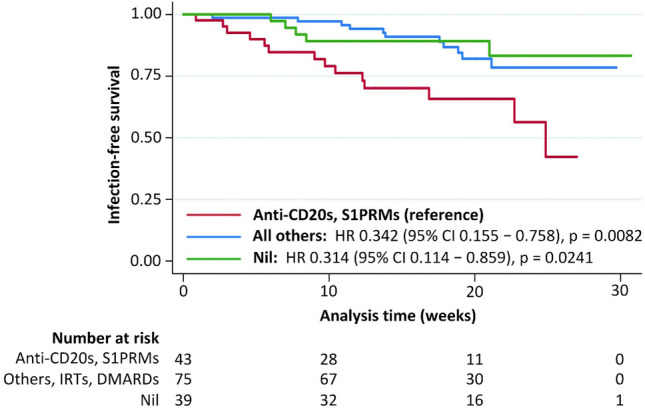
Two hundred and one patients were included; 47 had COVID-19 infection during the study period. Multivariable logistic regression revealed that receipt of a third SARS-CoV-2 mRNA vaccination (V3) was protective against COVID-19 infection. No particular immunotherapy group increased the risk of infection, however, Cox proportional-hazards regression showed that patients on anti-CD20s and sphingosine-1-phosphate modulators (S1PRMs) had a shorter time to infection after V3, compared to those on other immunotherapies or not on immunotherapy.
The Omicron subvariant BA.1/2 is highly infectious in patients with central nervous system inflammatory diseases; three doses of mRNA vaccination improved protection. However, treatment with anti-CD20s and S1PRMs predisposed patients to earlier infection. Future studies are required to determine the protective efficacy of newer bivalent vaccines that target the Omicron (sub)variant, especially in immunocompromised patients.
SARS-CoV-2 的奥密克戎变体似乎导致了较轻微的感染,然而,其免疫逃逸能力和高传染性(尽管已接种疫苗)仍然令人担忧,尤其是在免疫抑制患者中。在此,我们研究了 SARS-CoV-2 奥密克戎亚变体 BA.1/2 浪潮期间,新加坡接种疫苗的成年多发性硬化症 (MS)、水通道蛋白 4 抗体视神经脊髓炎谱系障碍 (AQP4-Ab NMOSD) 和髓鞘少突胶质细胞糖蛋白抗体相关疾病 (MOGAD) 患者的 COVID-19 感染发生率和危险因素。
这是在新加坡国家神经科学研究所进行的一项前瞻性观察性研究。仅纳入至少接种两剂 mRNA 疫苗的患者。收集人口统计学、疾病特征、COVID-19 感染和疫苗接种以及免疫疗法的数据。在接种疫苗后的不同时间点测量 SARS-CoV-2 中和抗体。
共纳入 210 例患者;研究期间有 47 例发生 COVID-19 感染。多变量逻辑回归显示,接种第三剂 SARS-CoV-2 mRNA 疫苗(V3)可预防 COVID-19 感染。没有特定的免疫治疗组会增加感染风险,然而,Cox 比例风险回归显示,与接受其他免疫疗法或未接受免疫疗法的患者相比,接受抗 CD20s 和鞘氨醇-1-磷酸调节剂 (S1PRMs) 的患者在接种 V3 后感染的时间更短。
奥密克戎亚变体 BA.1/2 在中枢神经系统炎症性疾病患者中具有高度传染性;三剂 mRNA 疫苗可提高保护效果。然而,抗 CD20s 和 S1PRMs 的治疗使患者更容易更早感染。需要进一步研究以确定针对奥密克戎(亚)变体的新型二价疫苗的保护效力,尤其是在免疫功能低下的患者中。