Section of Gastroenterology and Hepatology, West Virginia University School of Medicine, Morgantown.
Division of Gastroenterology and Hepatology, Johns Hopkins University School of Medicine, Baltimore, Maryland.
JAMA Netw Open. 2023 Apr 3;6(4):e237188. doi: 10.1001/jamanetworkopen.2023.7188.
Bariatric surgery (BS) is associated with significantly reduced incidence of cardiovascular diseases and mortality in patients with obesity. However, whether BS can decrease major adverse cardiovascular events in patients with nonalcoholic fatty liver disease (NAFLD) remains poorly understood.
To investigate the association of BS with the incidence of adverse cardiovascular events and all-cause mortality in patients with NAFLD and obesity.
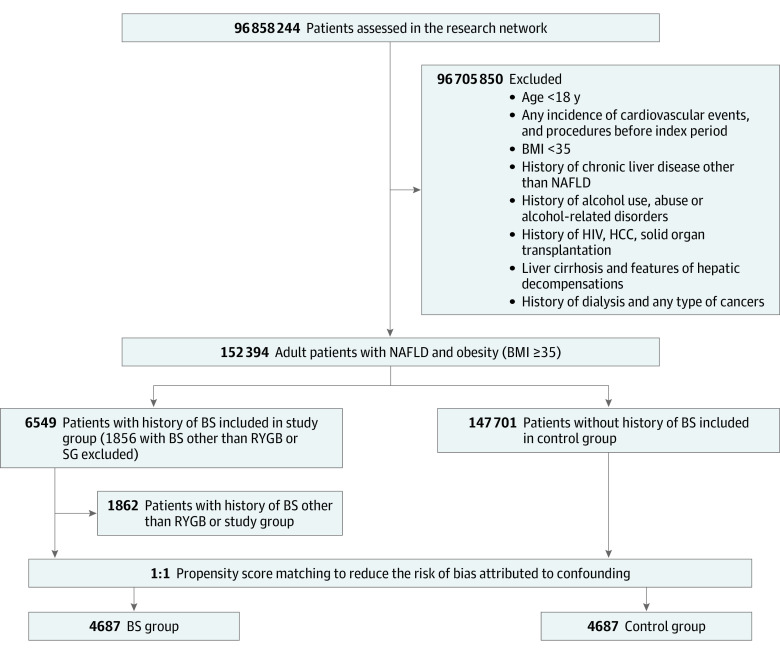
DESIGN, SETTING, AND PARTICIPANTS: This was a large, population-based, retrospective cohort using data from the TriNetX platform. Adult patients with a body mass index (BMI, calculated as weight in kilograms divided by height in meters squared) of 35 or greater and NAFLD (without cirrhosis) who underwent BS between January 1, 2005, and December 31, 2021, were included. Patients in the BS group were matched with patients who did not undergo surgery (non-BS group) according to age, demographics, comorbidities, and medication by using 1:1 propensity matching. Patient follow-up ended on August 31, 2022, and data were analyzed in September 2022.
Bariatric surgery vs nonsurgical care.
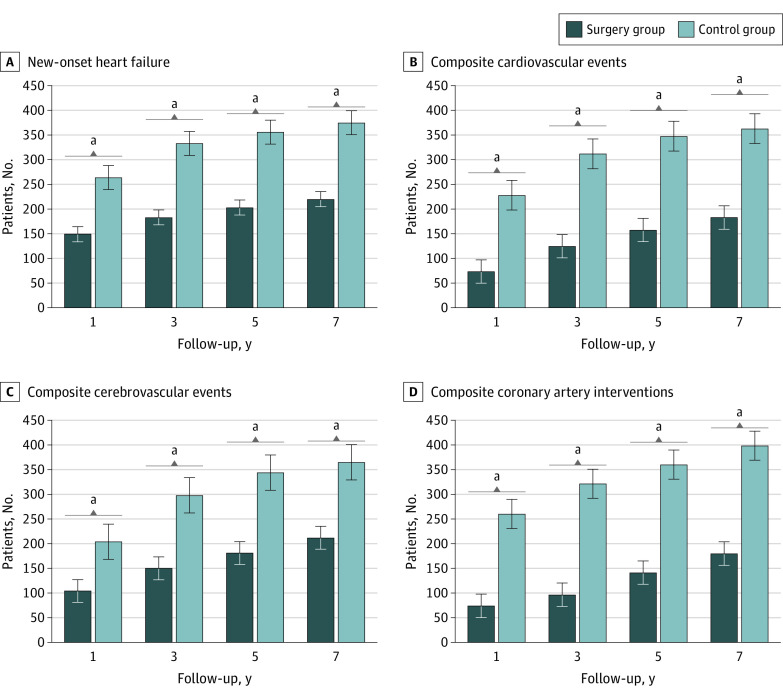
The primary outcomes were defined as the first incidence of new-onset heart failure (HF), composite cardiovascular events (unstable angina, myocardial infarction, or revascularization, including percutaneous coronary intervention or coronary artery bypass graft), composite cerebrovascular disease (ischemic or hemorrhagic stroke, cerebral infarction, transient ischemic attack, carotid intervention, or surgery), and a composite of coronary artery procedures or surgeries (coronary stenting, percutaneous coronary intervention, or coronary artery bypass). Cox proportional hazards models were used to estimate hazard ratios (HRs).
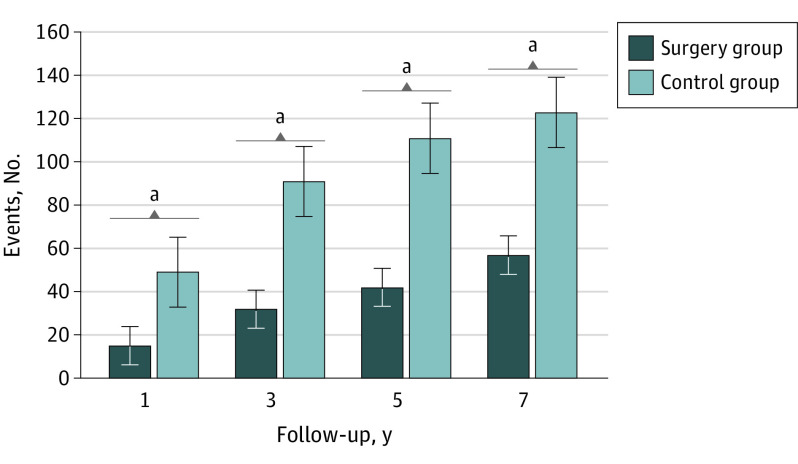
Of 152 394 eligible adults, 4693 individuals underwent BS; 4687 patients who underwent BS (mean [SD] age, 44.8 [11.6] years; 3822 [81.5%] female) were matched with 4687 individuals (mean [SD] age, 44.7 [13.2] years; 3883 [82.8%] years) who did not undergo BS. The BS group had significantly lower risk of new-onset of HF (HR, 0.60; 95% CI, 0.51-0.70), cardiovascular events (HR, 0.53; 95% CI, 0.44-0.65), cerebrovascular events (HR, 0.59; 95% CI, 0.51-0.69), and coronary artery interventions (HR, 0.47; 95% CI, 0.35-0.63) compared with the non-BS group. Similarly, all-cause mortality was substantially lower in the BS group (HR, 0.56; 95% CI, 0.42-0.74). These outcomes were consistent at follow-up duration of 1, 3, 5, and 7 years.
These findings suggest that BS was significantly associated with lower risk of major adverse cardiovascular events and all-cause mortality in patients with NAFLD and obesity.
减重手术(BS)与肥胖患者心血管疾病发生率和死亡率的显著降低相关。然而,BS 是否可以降低非酒精性脂肪性肝病(NAFLD)患者的主要不良心血管事件仍知之甚少。
研究 BS 与 NAFLD 和肥胖患者不良心血管事件和全因死亡率的相关性。
设计、设置和参与者:这是一项基于人群的大型回顾性队列研究,使用了来自 TriNetX 平台的数据。纳入 2005 年 1 月 1 日至 2021 年 12 月 31 日期间 BMI(体重以千克为单位除以身高以米为单位)为 35 或更高且患有 NAFLD(无肝硬化)并接受 BS 的成年患者。BS 组患者根据年龄、人口统计学特征、合并症和药物使用 1:1 倾向匹配与未接受手术的患者(非 BS 组)相匹配。患者随访于 2022 年 8 月 31 日结束,数据于 2022 年 9 月进行分析。
BS 与非手术治疗。
主要结局定义为新发心力衰竭(HF)、复合心血管事件(不稳定型心绞痛、心肌梗死或血运重建,包括经皮冠状动脉介入治疗或冠状动脉旁路移植术)、复合脑血管疾病(缺血性或出血性中风、脑梗死、短暂性脑缺血发作、颈动脉介入或手术)和冠状动脉手术或血运重建的复合终点(冠状动脉支架置入术、经皮冠状动脉介入治疗或冠状动脉旁路移植术)的首次发生。Cox 比例风险模型用于估计风险比(HR)。
在 152394 名合格成年人中,4693 人接受了 BS;4687 名接受 BS(平均[SD]年龄,44.8[11.6]岁;3822[81.5%]为女性)的患者与 4687 名未接受 BS(平均[SD]年龄,44.7[13.2]岁;3883[82.8%]岁)的患者相匹配。BS 组新发 HF(HR,0.60;95%CI,0.51-0.70)、心血管事件(HR,0.53;95%CI,0.44-0.65)、脑血管事件(HR,0.59;95%CI,0.51-0.69)和冠状动脉介入治疗(HR,0.47;95%CI,0.35-0.63)的风险明显较低。同样,BS 组的全因死亡率也明显较低(HR,0.56;95%CI,0.42-0.74)。在 1、3、5 和 7 年的随访中,这些结果都是一致的。
这些发现表明,BS 与 NAFLD 和肥胖患者的主要不良心血管事件和全因死亡率降低显著相关。