Department of Biomedical Informatics, College of Medicine, The Ohio State University, Columbus.
Secondary Data Core, Center for Biostatistics, College of Medicine, The Ohio State University, Columbus.
JAMA Netw Open. 2022 Oct 3;5(10):e2235003. doi: 10.1001/jamanetworkopen.2022.35003.
There are no approved treatments for nonalcoholic fatty liver disease (NAFLD) despite its association with obesity and increased risk of cardiovascular disease (CVD).
To examine the association between bariatric surgery and CVD risk in individuals with severe obesity and NAFLD.
DESIGN, SETTING, AND PARTICIPANTS: This large, population-based retrospective cohort study obtained data from the MarketScan Commercial Claims and Encounters database from January 1, 2007, to December 31, 2017. Participants included insured adults aged 18 to 64 years with NAFLD and severe obesity (body mass index ≥40) without a history of bariatric surgery or CVD before NAFLD diagnosis. Baseline characteristics were balanced between individuals who underwent surgery (surgical group) and those who did not (nonsurgical group) using inverse probability of treatment weighting. Data were analyzed from March 2020 to April 2021.
Bariatric surgery (Roux-en-Y gastric bypass, sleeve gastrectomy, and other bariatric procedures) vs nonsurgical care.
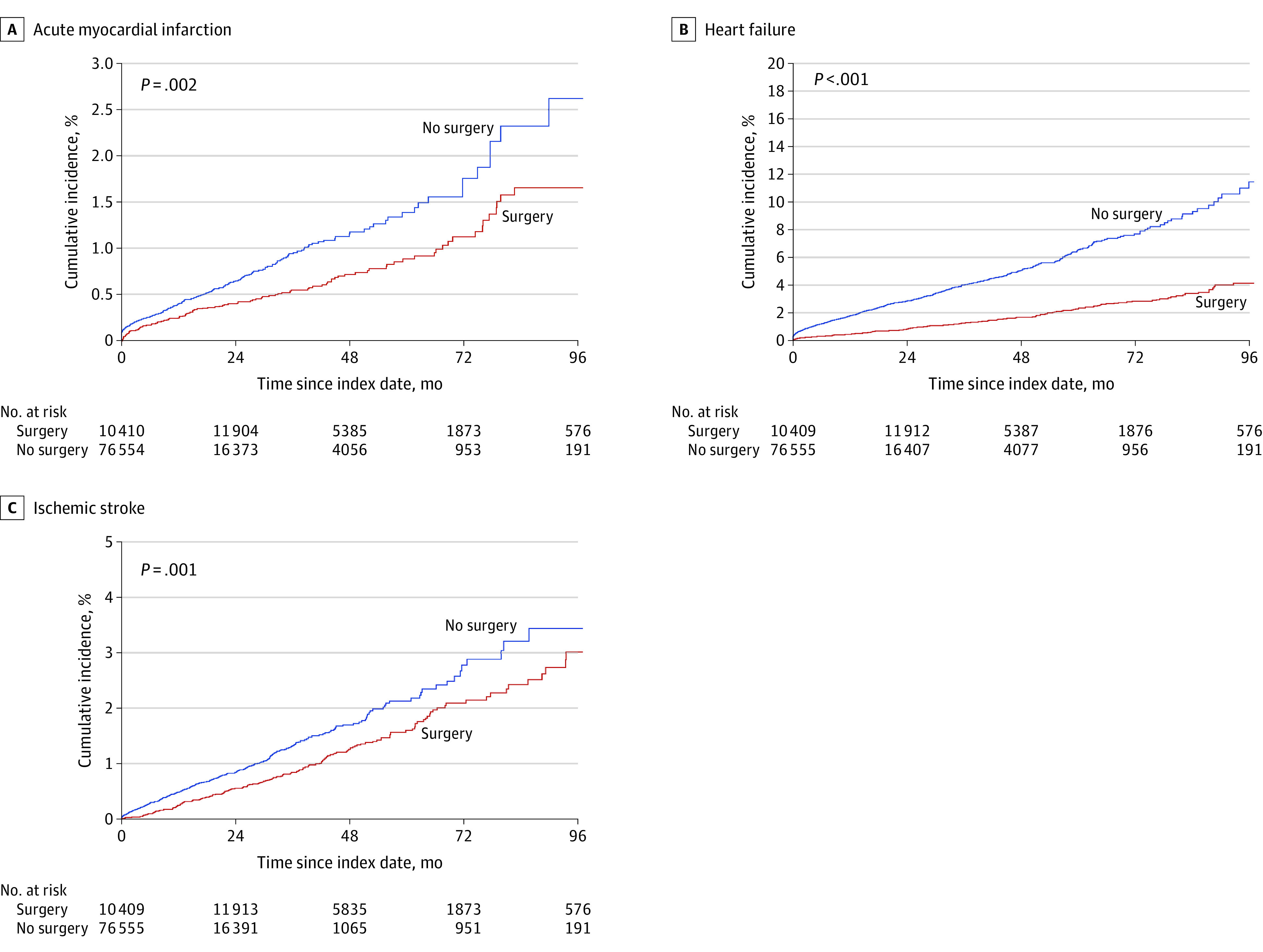
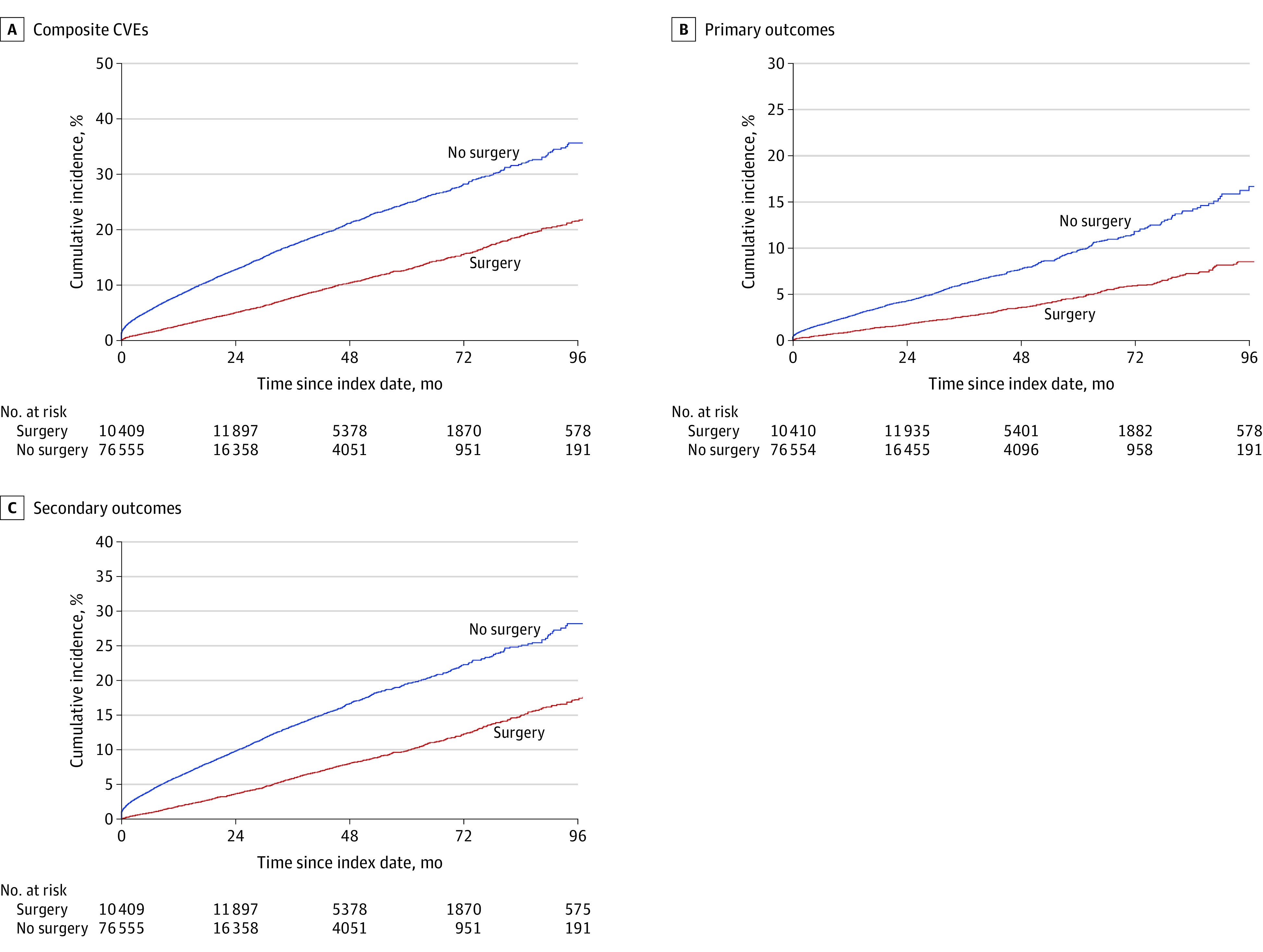
The main outcome was the incidence of cardiovascular events (primary or secondary composite CVD outcomes). The primary composite outcome included myocardial infarction, heart failure, or ischemic stroke, and the secondary composite outcome included secondary ischemic heart events, transient ischemic attack, secondary cerebrovascular events, arterial embolism and thrombosis, or atherosclerosis. Cox proportional hazards regression models with inverse probability treatment weighting were used to examine the associations between bariatric surgery, modeled as time varying, and all outcomes.
The study included 86 964 adults (mean [SD] age, 44.3 [10.9] years; 59 773 women [68.7%]). Of these individuals, 30 300 (34.8%) underwent bariatric surgery and 56 664 (65.2%) received nonsurgical care. All baseline covariates were balanced after applying inverse probability treatment weighting. In the surgical group, 1568 individuals experienced incident cardiovascular events compared with 7215 individuals in the nonsurgical group (incidence rate difference, 4.8 [95% CI, 4.5-5.0] per 100 person-years). At the end of the study, bariatric surgery was associated with a 49% lower risk of CVD (adjusted hazard ratio [aHR], 0.51; 95% CI, 0.48-0.54) compared with nonsurgical care. The risk of primary composite CVD outcomes was reduced by 47% (aHR, 0.53 [95% CI, 0.48-0.59), and the risk of secondary composite CVD outcomes decreased by 50% (aHR, 0.50; 95% CI, 0.46-0.53) in individuals with vs without surgery.
Results of this study suggest that, compared with nonsurgical care, bariatric surgery was associated with significant reduction in CVD risk in individuals with severe obesity and NAFLD.
尽管非酒精性脂肪性肝病(NAFLD)与肥胖和心血管疾病(CVD)风险增加有关,但目前尚无针对其的批准治疗方法。
研究减重手术与严重肥胖和 NAFLD 患者 CVD 风险之间的关系。
设计、地点和参与者:这是一项大型的基于人群的回顾性队列研究,从 2007 年 1 月 1 日至 2017 年 12 月 31 日,从 MarketScan 商业索赔和就诊数据库中获取数据。参与者包括年龄在 18 至 64 岁之间、患有严重肥胖症(BMI≥40)和 NAFLD 的有保险成年人,并且在 NAFLD 诊断前无减重手术或 CVD 病史。通过逆概率治疗加权法,在接受手术(手术组)和未接受手术(非手术组)的个体之间平衡基线特征。数据于 2020 年 3 月至 2021 年 4 月进行分析。
减重手术(Roux-en-Y 胃旁路术、袖状胃切除术和其他减重手术)与非手术治疗。
主要结果是心血管事件的发生率(主要或次要复合 CVD 结局)。主要复合结局包括心肌梗死、心力衰竭或缺血性中风,次要复合结局包括二级缺血性心脏病事件、短暂性脑缺血发作、二级脑血管事件、动脉栓塞和血栓形成或动脉粥样硬化。使用逆概率治疗加权的 Cox 比例风险回归模型来检查减重手术(作为时间变化的因素)与所有结局之间的关系。
该研究纳入了 86964 名成年人(平均[标准差]年龄为 44.3[10.9]岁;59773 名女性[68.7%])。其中,30300 名(34.8%)接受了减重手术,56664 名(65.2%)接受了非手术治疗。所有基线协变量在应用逆概率治疗加权后均达到平衡。在手术组中,有 1568 名患者发生了心血管事件,而非手术组中有 7215 名患者发生了心血管事件(发生率差异,每 100 人年 4.8[95%CI,4.5-5.0])。研究结束时,与非手术治疗相比,减重手术使 CVD 风险降低了 49%(校正后的危险比[HR],0.51;95%CI,0.48-0.54)。与无手术治疗相比,主要复合 CVD 结局的风险降低了 47%(HR,0.53[95%CI,0.48-0.59),次要复合 CVD 结局的风险降低了 50%(HR,0.50[95%CI,0.46-0.53)。
这项研究的结果表明,与非手术治疗相比,减重手术与严重肥胖和 NAFLD 患者的 CVD 风险显著降低相关。