Park Dae Hyoung, Yu Ji Hyeong
Department of Urology, INJE University Sanggye Paik Hospital, Seoul, Republic of Korea.
Transl Cancer Res. 2023 Mar 31;12(3):502-514. doi: 10.21037/tcr-22-1855. Epub 2023 Mar 17.
Evaluation of prostate cancer (PCa) when serum prostate-specific antigen (PSA) level is vaguely elevated is complicated. This is because serum PSA levels only reflect the number of prostate epithelial cells. We aimed to compare PSA and various prostate volume-related factors to determine which one can best predict PCa in patients with a PSA level of 2.5-20 ng/mL.
Patients who underwent transrectal ultrasound (TRUS)-guided prostate biopsy at the Inje University Sanggye Paik Hospital between January 2018 and July 2021 and who had a PSA level of 2.5-20 ng/mL were retrospectively identified (n=275). Among them, based on biopsy results, patients were divided into cancer group and non-cancer groups, and age, PSA, total prostate volume (TPV), peripheral zone volume (PZV), peripheral zone PSA density (PZ-PSAD), transitional zone-PSAD (TZ-PSAD), and PSAD were compared and analyzed using receiver operating characteristic (ROC) and univariate analyses.
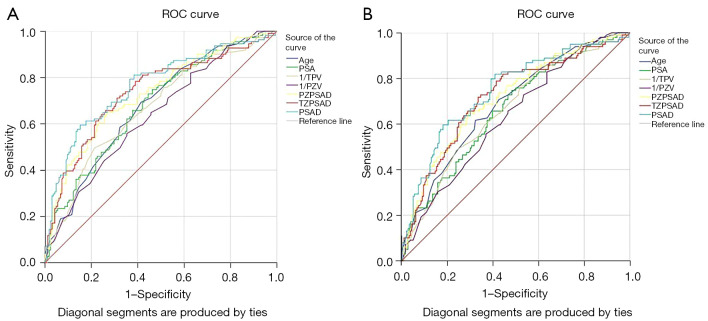
The areas under ROC curves (AUCs) for age, total PSA, TPV, PZV, PZ-PSAD, TZ-PSAD, and PSAD for predicting PCa in patients with a PSA level of 2.5-20.0 ng/mL were 0.678, 0.680, 0.671, 0.639, 0.731, 0.736, and 0.764, respectively. In univariate and multivariate analysis, all categorical variables were divided based on the cut-off value and used to predict PCa. Those with a PSAD of ≥0.218 ng/mL were found to be at an increased risk of PCa than those with a PSAD of <0.218 ng/mL [odds ratio (OR) =3.51; 95% confidence interval (CI): 1.306-9.415], which was the best result, followed by TZ-PSAD with a cut-off value of 0.353. At a PSAD level of 0.218 ng/mL, 85.0% of the PCa group could avoid unnecessary biopsy and 61.4% of the non-PCa group could reduce missed diagnosis when the TRUS findings were inaccurate.
PSAD may inform biopsy decisions as the best predictor of PCa when TRUS findings are ambiguous in patients with a PSA level of 2.5-20.0 ng/mL.
当血清前列腺特异性抗原(PSA)水平轻度升高时,前列腺癌(PCa)的评估较为复杂。这是因为血清PSA水平仅反映前列腺上皮细胞数量。我们旨在比较PSA与各种前列腺体积相关因素,以确定哪一个能最好地预测PSA水平在2.5 - 20 ng/mL的患者是否患有PCa。
回顾性纳入2018年1月至2021年7月在仁济大学桑格耶白医院接受经直肠超声(TRUS)引导下前列腺穿刺活检且PSA水平在2.5 - 20 ng/mL的患者(n = 275)。其中,根据活检结果将患者分为癌症组和非癌症组,比较并分析年龄、PSA、前列腺总体积(TPV)、外周带体积(PZV)、外周带PSA密度(PZ - PSAD)、移行带PSA密度(TZ - PSAD)和PSAD,采用受试者工作特征(ROC)曲线和单因素分析。
对于PSA水平在2.5 - 20.0 ng/mL的患者,年龄、总PSA、TPV、PZV、PZ - PSAD、TZ - PSAD和PSAD预测PCa的ROC曲线下面积(AUC)分别为0.678、0.680、0.671、0.639、0.731、0.736和0.764。在单因素和多因素分析中,所有分类变量均根据临界值进行划分并用于预测PCa。发现PSAD≥0.218 ng/mL的患者患PCa的风险高于PSAD<0.218 ng/mL的患者[比值比(OR)= 3.51;95%置信区间(CI):1.306 - 9.415],这是最佳结果,其次是临界值为0.353的TZ - PSAD。当PSAD水平为0.218 ng/mL时,在TRUS检查结果不准确的情况下,PCa组中85.0%的患者可避免不必要的活检,非PCa组中61.4%的患者可减少漏诊。
当PSA水平在2.5 - 20.0 ng/mL的患者TRUS检查结果不明确时,PSAD可能作为PCa的最佳预测指标,为活检决策提供参考。