Bohac Maja, Jagic Mateja, Biscevic Alma, Lukacevic Selma, Mravicic Ivana, Suic Smiljka Popovic, Dekaris Iva
University Eye Hospital Svjetlost, School of Medicine University of Rijeka, Zagreb, Croatia.
Eye Clinic Svjetlost, Sarajevo, Bosnia and Herzegovina.
Acta Inform Med. 2023 Mar;31(1):62-67. doi: 10.5455/aim.2023.31.62-67.
Among various visual functions, stereoacuity, or the ability to perceive depth, is the most sophisticated binocular function. Many publications discuss the influence of retinal image formation by multifocal intraocular lenses on glare and contrast sensitivity, but only a few present results of testing binocular vision in patients with multifocal intraocular lenses.
This article is designed to review the results of testing binocular vision in patients with multifocal intraocular lenses implanted in cataract surgery.
This article was performed based on a literature review and Internet search through scientific databases such as PubMed, Scopus, Web of Science, and Google Scholar.
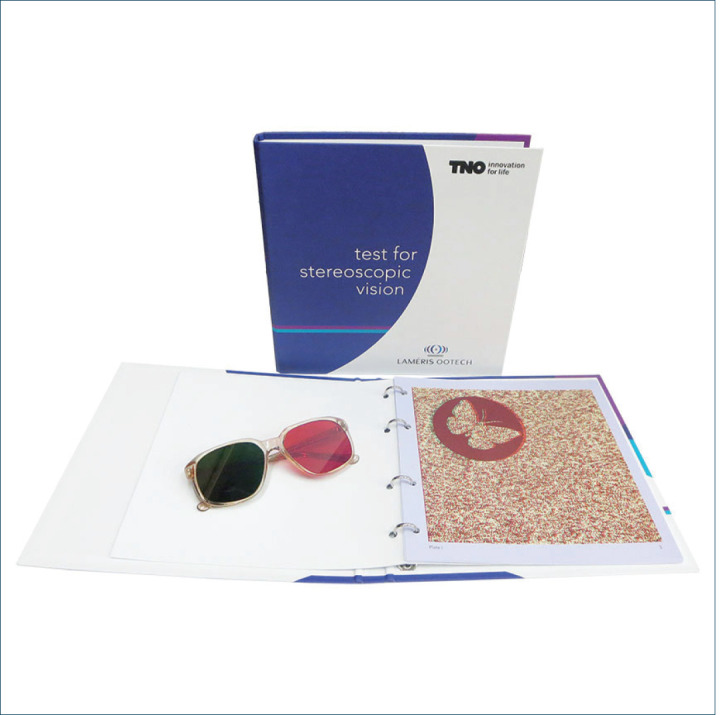
Some reports found that patients implanted with the monofocal lens, when measured with a near addition, presented statistically significant better stereoacuity scores than those implanted with any of the multifocal intraocular lens types. When the TNO test was used for measurement, statistically significant better stereoacuity was disclosed with the refractive multifocal intraocular lens than with the diffractive-based multifocal intraocular lens design. Stereoacuity scores, even within the same types of lenses, were significantly better with the Titmus test than with the TNO test.
Stereoacuity is not affected by multifocality-induced retinal blur as it is by other causes of image degradation such as small residual refractive error very early opacification of ocular media or dry eye. Multifocal intraocular lenses do not cause more functional aniseikonia than would be expected with a monofocal intraocular lens. Since stereoacuity is compromised with unilateral multifocal intraocular lens implantation bilateral implantation should be attempted.
在各种视觉功能中,立体视锐度,即感知深度的能力,是最复杂的双眼功能。许多出版物讨论了多焦点人工晶状体对视网膜成像的影响,包括眩光和对比敏感度,但只有少数研究给出了多焦点人工晶状体患者双眼视觉测试的结果。
本文旨在综述白内障手术中植入多焦点人工晶状体患者的双眼视觉测试结果。
本文基于文献综述以及通过PubMed、Scopus、Web of Science和谷歌学术等科学数据库进行的互联网搜索完成。
一些报告发现,单焦点人工晶状体植入患者在使用近附加镜测量时,其立体视锐度得分在统计学上显著高于任何一种多焦点人工晶状体植入患者。当使用TNO测试进行测量时,屈光性多焦点人工晶状体的立体视锐度在统计学上显著优于衍射型多焦点人工晶状体设计。即使在同一类型的晶状体中,Titmus测试的立体视锐度得分也显著优于TNO测试。
立体视锐度不受多焦点引起的视网膜模糊影响,不像其他图像退化原因那样,如微小残余屈光不正、眼内介质早期混浊或干眼。多焦点人工晶状体不会比单焦点人工晶状体导致更多功能性像不等。由于单侧植入多焦点人工晶状体时立体视锐度会受损,因此应尝试双侧植入。