Reiker Theresa, Des Rosiers Sarah, Boch Johannes, Partha Gautam, Venkitachalam Lakshmi, Santana Adela, Srivasatava Abhinav, Barboza Joseph, Byambasuren Enkhtuya, Baxter Yara C, Dib Karina Mauro, Dashdorj Naranjargal, Anne Malick, de Oliveira Renato W, Silveira Mariana, Ferrer Jose M E, Morgan Louise, Jones Olivia, Luvsansambuu Tumurbaatar, Bortolotto Luiz Aparecido, Drager Luciano, Avezum Alvaro, Aerts Ann
Novartis Foundation, Basel, Switzerland.
Novartis Healthcare Pvt. Ltd., Hyderabad, India.
PLOS Glob Public Health. 2023 Apr 11;3(4):e0001480. doi: 10.1371/journal.pgph.0001480. eCollection 2023.
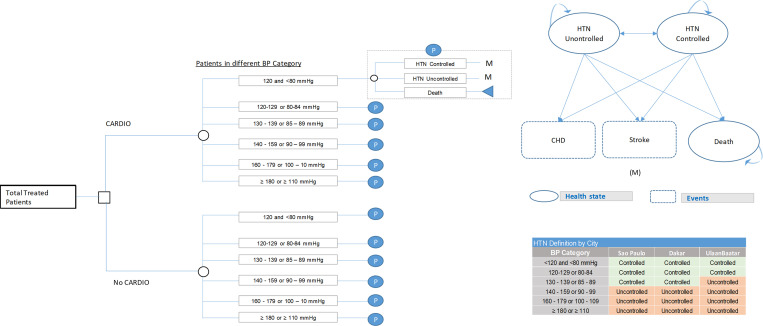
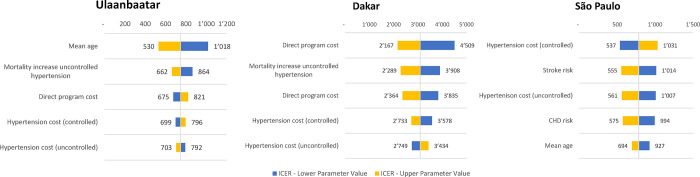
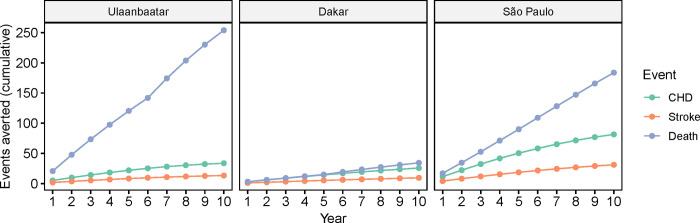
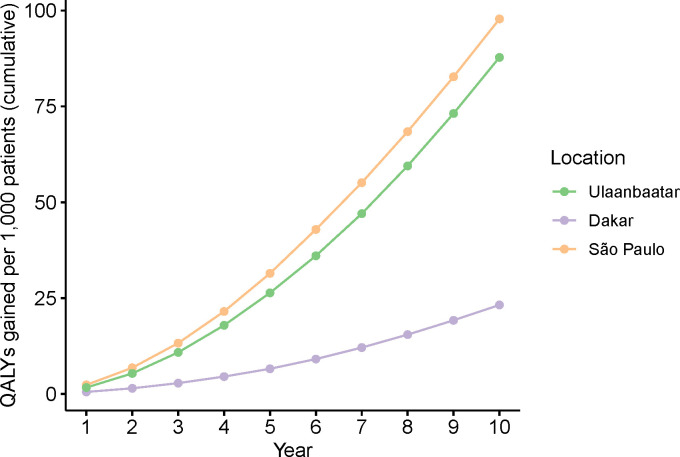
Cardiovascular disease (CVD) is the leading cause of mortality worldwide, with 80% of that mortality occurring in low- and middle-income countries. Hypertension, its primary risk factor, can be effectively addressed through multisectoral, multi-intervention initiatives. However, evidence for the population-level impact on cardiovascular (CV) event rates and mortality, and the cost-effectiveness of such initiatives is scarce as long-term longitudinal data is often lacking. Here, we model the long-term population health impact and cost-effectiveness of a multisectoral urban population health initiative designed to reduce hypertension, conducted in Ulaanbaatar (Mongolia), Dakar (Senegal), and in the district of Itaquera in São Paulo (Brazil) in collaboration with the local governments. We based our analysis on cohort-level data among hypertensive patients on treatment and control rates from a real-world effectiveness study of the CARDIO4Cities approach (built on quality of care, early access, policy reform, data and digital, Intersectoral collaboration, and local ownership). We built a decision tree model to estimate the CV event rates during implementation (1-2 years) and a Markov model to project health outcomes over 10 years. We estimated the number of CV events averted and quality-adjusted life-years gained (QALYs through the initiative and assessed its cost-effectiveness based on the costs reported by the funder using the incremental cost effectiveness ratio (ICER) and published thresholds. A one-way sensitivity analysis was performed to assess the robustness of the results. The modelled patient cohorts included 10,075 patients treated for hypertension in Ulaanbaatar, 5,236 in Dakar, and 5,844 in São Paulo. We estimated that 3.3-12.8% of strokes and 3.0-12.0% of coronary heart disease (CHD) events were averted during 1-2 years of implementation in the three cities. We estimated that over the subsequent 10 years, 3.6-9.9% of strokes, 2.8-7.8% of CHD events, and 2.7-7.9% of premature deaths would be averted. The estimated ICER was USD 748 QALY gained in Ulaanbaatar, USD 3091 in Dakar, and USD 784 in São Paulo. With that, the intervention was estimated to be cost-effective in Ulaanbaatar and São Paulo. For Dakar, cost-effectiveness was met under WHO-CHOICE standards, but not under more conservative standards adjusted for purchasing power parity (PPP) and opportunity costs. The findings were robust to the sensitivity analysis. Our results provide evidence that the favorable impact of multisector systemic interventions designed to reduce the hypertension burden extend to long-term population-level CV health outcomes and are likely cost-effective. The CARDIO4Cities approach is predicted to be a cost-effective solution to alleviate the growing CVD burden in cities across the world.
心血管疾病(CVD)是全球主要死因,其中80%的死亡发生在低收入和中等收入国家。高血压作为其主要风险因素,可通过多部门、多干预举措有效应对。然而,由于往往缺乏长期纵向数据,此类举措对心血管(CV)事件发生率和死亡率的人群层面影响以及成本效益的证据很少。在此,我们模拟了一项与当地政府合作在乌兰巴托(蒙古)、达喀尔(塞内加尔)以及圣保罗的伊塔夸拉区(巴西)开展的旨在降低高血压的多部门城市人群健康倡议的长期人群健康影响和成本效益。我们的分析基于一项关于CARDIO4Cities方法(基于医疗质量、早期就医、政策改革、数据与数字、部门间协作以及地方自主权)的真实世界有效性研究中高血压患者治疗和控制率的队列层面数据。我们构建了一个决策树模型来估计实施期间(1至2年)的CV事件发生率,并构建了一个马尔可夫模型来预测10年的健康结果。我们估计了通过该倡议避免的CV事件数量以及获得的质量调整生命年(QALY),并根据资助者报告的成本,使用增量成本效益比(ICER)和已公布的阈值评估其成本效益。进行了单向敏感性分析以评估结果的稳健性。模拟的患者队列包括乌兰巴托10,075名接受高血压治疗的患者、达喀尔5,236名以及圣保罗5,844名。我们估计在这三个城市实施的1至2年内,可避免3.3%至12.8%的中风和3.0%至12.0%的冠心病(CHD)事件。我们估计在随后的10年中,可避免3.6%至9.9%的中风、2.8%至7.8%的CHD事件以及2.7%至7.9%的过早死亡。估计的ICER在乌兰巴托为每获得一个QALY 748美元,在达喀尔为3091美元,在圣保罗为784美元。据此,该干预措施在乌兰巴托和圣保罗估计具有成本效益。对于达喀尔,按照世界卫生组织的CHOICE标准符合成本效益,但按照根据购买力平价(PPP)和机会成本调整的更保守标准则不符合。研究结果对敏感性分析具有稳健性。我们的结果提供了证据,表明旨在减轻高血压负担的多部门系统性干预措施的有利影响可扩展至长期人群层面的CV健康结果,并且可能具有成本效益。预计CARDIO4Cities方法是减轻全球城市日益增长的CVD负担的一种具有成本效益的解决方案。