Laboratory for Leukemia Diagnostics, Department of Medicine III, University Hospital, LMU Munich, Munich, Germany.
Institute of Human Genetics, University Hospital, LMU Munich, Munich, Germany.
Leukemia. 2023 Jun;37(6):1234-1244. doi: 10.1038/s41375-023-01884-2. Epub 2023 Apr 11.
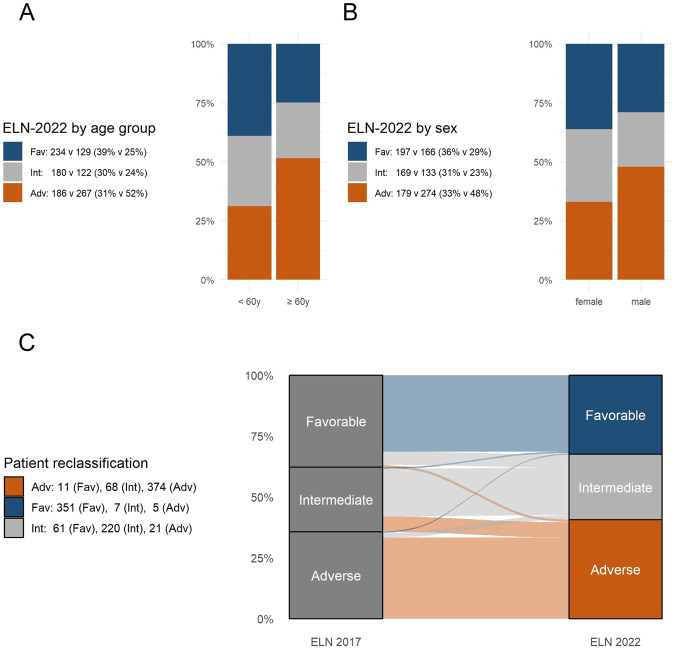
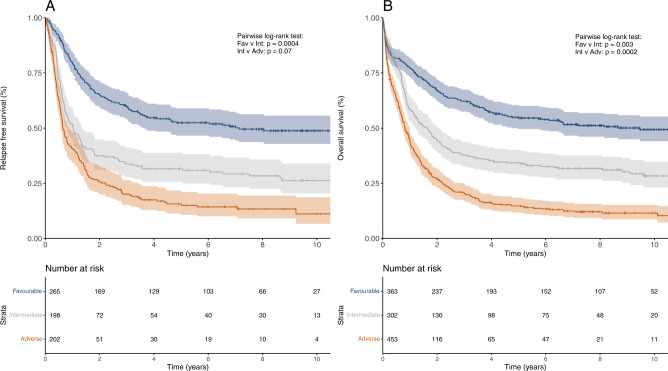
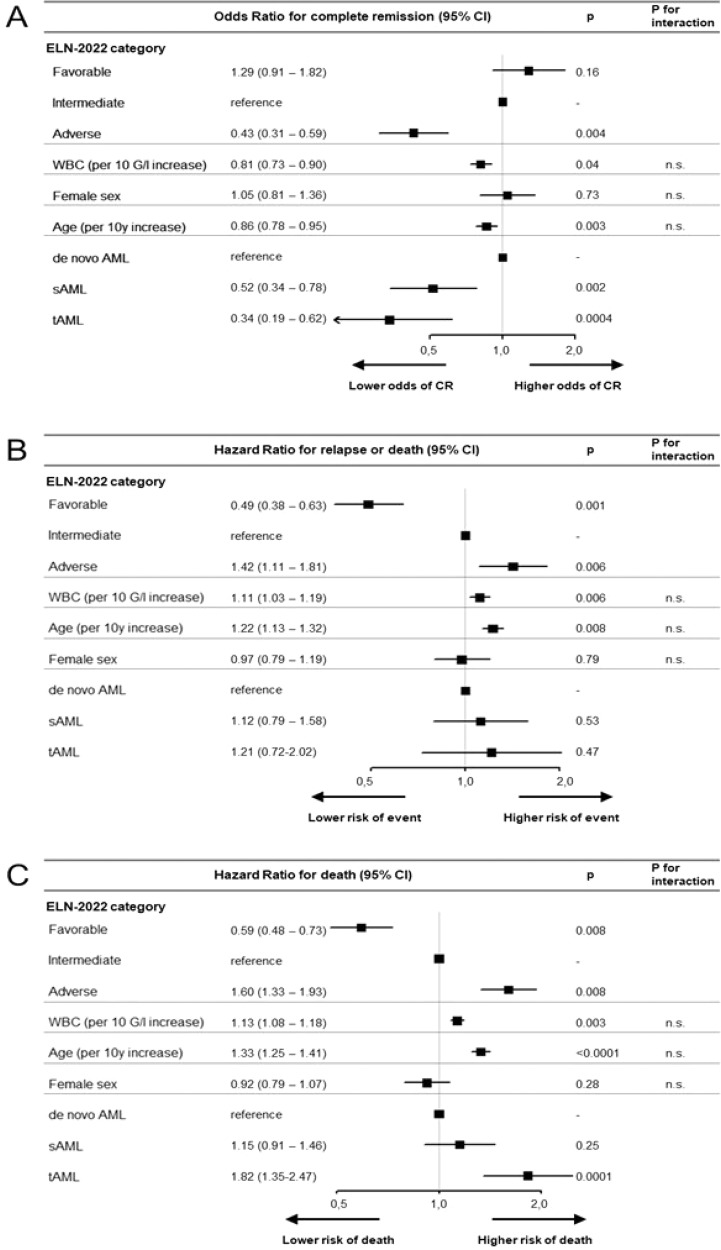
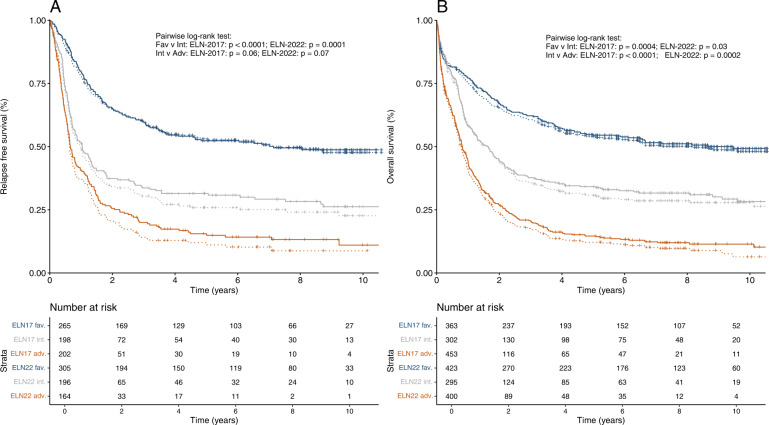
The revised 2022 European LeukemiaNet (ELN) AML risk stratification system requires validation in large, homogeneously treated cohorts. We studied 1118 newly diagnosed AML patients (median age, 58 years; range, 18-86 years) who received cytarabine-based induction chemotherapy between 1999 and 2012 and compared ELN-2022 to the previous ELN-2017 risk classification. Key findings were validated in a cohort of 1160 mostly younger patients. ELN-2022 reclassified 15% of patients, 3% into more favorable, and 12% into more adverse risk groups. This was mainly driven by patients reclassified from intermediate- to adverse-risk based on additional myelodysplasia-related mutations being included as adverse-risk markers. These patients (n = 79) had significantly better outcomes than patients with other adverse-risk genotypes (5-year OS, 26% vs. 12%) and resembled the remaining intermediate-risk group. Overall, time-dependent ROC curves and Harrel's C-index controlling for age, sex, and AML type (de novo vs. sAML/tAML) show slightly worse prognostic discrimination of ELN-2022 compared to ELN-2017 for OS. Further refinement of ELN-2022 without including additional genetic markers is possible, in particular by recognizing TP53-mutated patients with complex karyotypes as "very adverse". In summary, the ELN-2022 risk classification identifies a larger group of adverse-risk patients at the cost of slightly reduced prognostic accuracy compared to ELN-2017.
修订后的 2022 年欧洲白血病网络(ELN)急性髓系白血病(AML)风险分层系统需要在大规模、同质治疗队列中进行验证。我们研究了 1118 例新诊断的 AML 患者(中位年龄 58 岁;范围 18-86 岁),他们在 1999 年至 2012 年期间接受了基于阿糖胞苷的诱导化疗,并将 ELN-2022 与之前的 ELN-2017 风险分类进行了比较。关键发现已在一组 1160 例主要为年轻患者的队列中得到验证。ELN-2022 重新分类了 15%的患者,其中 3%进入更有利的风险组,12%进入更不利的风险组。这主要是由于根据纳入的骨髓增生异常相关突变将中间风险患者重新分类为不利风险组。这些患者(n=79)的结局明显优于其他不利风险基因型的患者(5 年 OS,26% vs. 12%),与其余中间风险组相似。总体而言,时间依赖性 ROC 曲线和控制年龄、性别和 AML 类型(初发 vs. sAML/tAML)的 Harrell's C 指数显示,ELN-2022 对 OS 的预后判别能力略逊于 ELN-2017。进一步细化 ELN-2022 而不包括其他遗传标志物是可能的,特别是将具有复杂核型的 TP53 突变患者识别为“非常不利”。总之,ELN-2022 风险分类确定了更大比例的不利风险患者,但其预后准确性略低于 ELN-2017。