Ashford and Saint Peter's Hospitals NHS Trust, Chertsey, UK
Imperial College, London, UK.
BMJ Open. 2023 Apr 13;13(4):e068179. doi: 10.1136/bmjopen-2022-068179.
To evaluate the clinical efficacy and safety of leflunomide (L) added to the standard-of-care (SOC) treatment in COVID-19 patients hospitalised with moderate/critical clinical symptoms.
Prospective, open-label, multicentre, stratified, randomised clinical trial.
Five hospitals in UK and India, from September 2020 to May 2021.
Adults with PCR confirmed COVID-19 infection with moderate/critical symptoms within 15 days of onset.
Leflunomide 100 mg/day (3 days) followed by 10-20 mg/day (7 days) added to standard care.
The time to clinical improvement (TTCI) defined as two-point reduction on a clinical status scale or live discharge prior to 28 days; safety profile measured by the incidence of adverse events (AEs) within 28 days.
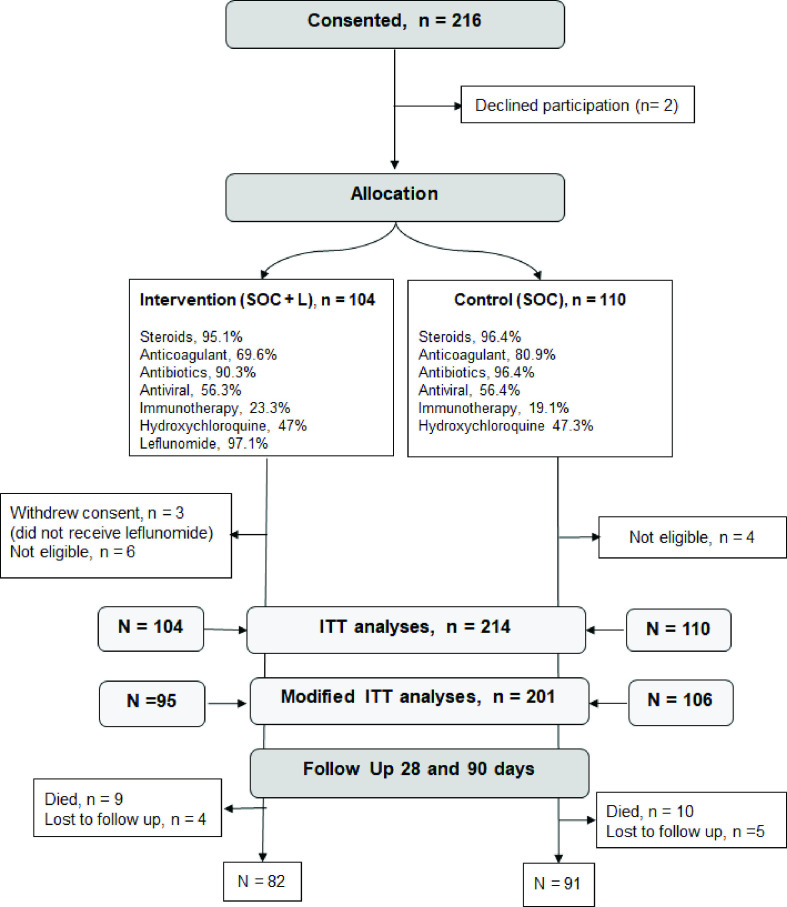
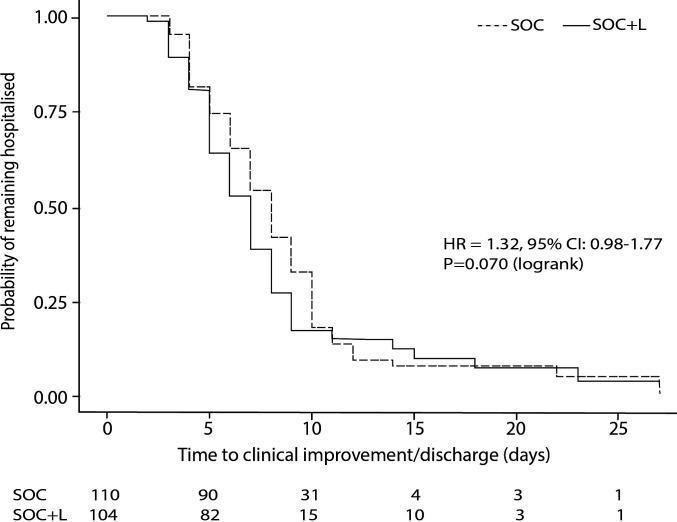
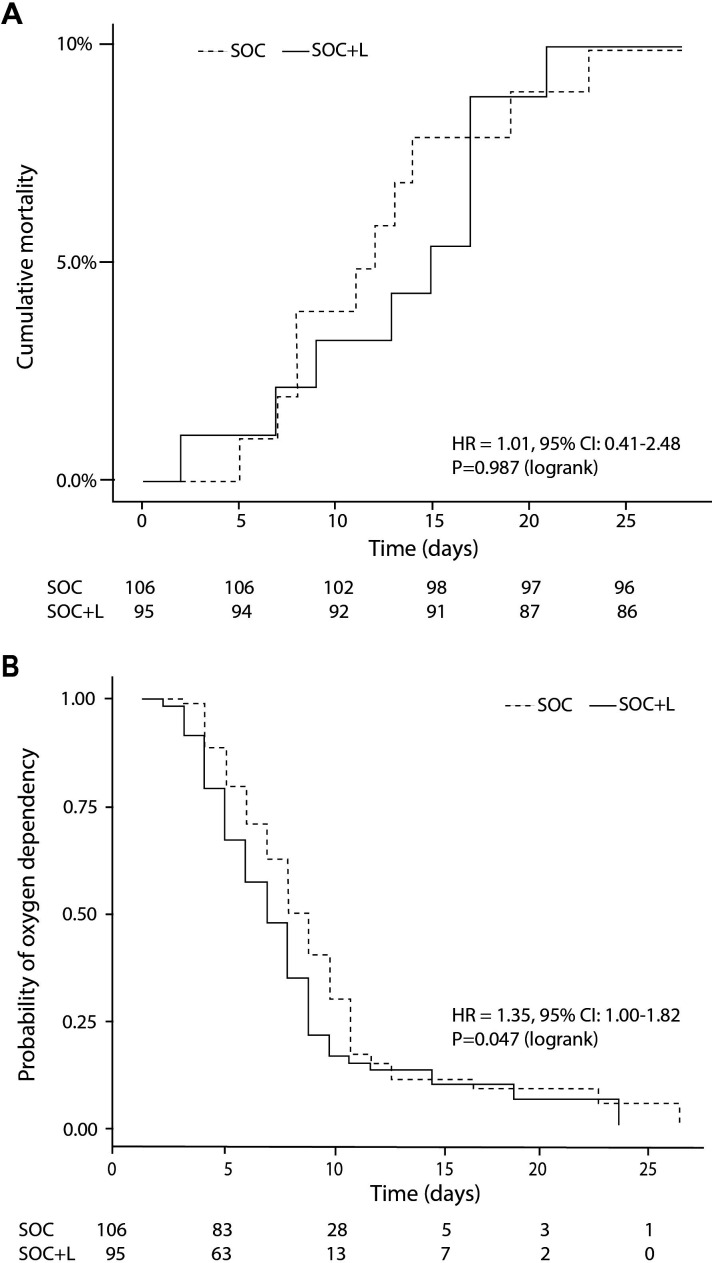
Eligible patients (n=214; age 56.3±14.9 years; 33% female) were randomised to SOC+L (n=104) and SOC group (n=110), stratified according to their clinical risk profile. TTCI was 7 vs 8 days in SOC+L vs SOC group (HR 1.317; 95% CI 0.980 to 1.768; p=0.070). Incidence of serious AEs was similar between the groups and none was attributed to leflunomide. In sensitivity analyses, excluding 10 patients not fulfilling the inclusion criteria and 3 who withdrew consent before leflunomide treatment, TTCI was 7 vs 8 days (HR 1.416, 95% CI 1.041 to 1.935; p=0.028), indicating a trend in favour of the intervention group. All-cause mortality rate was similar between groups, 9/104 vs 10/110. Duration of oxygen dependence was shorter in the SOC+L group being a median 6 days (IQR 4-8) compared with 7 days (IQR 5-10) in SOC group (p=0.047).
Leflunomide, added to the SOC treatment for COVID-19, was safe and well tolerated but had no major impact on clinical outcomes. It may shorten the time of oxygen dependence by 1 day and thereby improve TTCI/hospital discharge in moderately affected COVID-19 patients.
EudraCT Number: 2020-002952-18, NCT05007678.
评估来氟米特(L)联合标准治疗(SOC)用于治疗有中度/重症临床症状的 COVID-19 住院患者的临床疗效和安全性。
前瞻性、开放标签、多中心、分层、随机临床试验。
英国和印度的五家医院,时间为 2020 年 9 月至 2021 年 5 月。
PCR 确诊的 COVID-19 感染,发病 15 天内出现中度/重症症状的成年人。
来氟米特 100mg/天(3 天),随后每天 10-20mg(7 天),联合标准治疗。
临床改善时间(TTCI)定义为临床状态评分降低 2 分或在 28 天前出院;通过 28 天内不良事件(AE)的发生率来衡量安全性。
符合条件的患者(n=214;年龄 56.3±14.9 岁;33%为女性)按照其临床风险状况分层,随机分为 SOC+L 组(n=104)和 SOC 组(n=110)。SOC+L 组和 SOC 组的 TTCI 分别为 7 天和 8 天(HR 1.317;95%CI 0.980 至 1.768;p=0.070)。两组严重 AE 的发生率相似,均与来氟米特无关。在敏感性分析中,排除 10 名不符合纳入标准的患者和 3 名在接受来氟米特治疗前撤回同意的患者,TTCI 为 7 天和 8 天(HR 1.416,95%CI 1.041 至 1.935;p=0.028),表明干预组有获益趋势。两组的全因死亡率相似,分别为 9/104 和 10/110。SOC+L 组的氧依赖持续时间更短,中位数为 6 天(IQR 4-8),SOC 组为 7 天(IQR 5-10)(p=0.047)。
来氟米特联合 SOC 治疗 COVID-19 是安全且耐受良好的,但对临床结局没有显著影响。它可能使中度 COVID-19 患者的氧依赖时间缩短 1 天,从而改善 TTCI/出院。
EudraCT 编号:2020-002952-18,NCT05007678。