Llanos Jiménez Lucía, Alvarez-Alvarez Beatriz, Fonseca Aizpuru Eva, Peces-Barba Germán, Pindao Quesada Gloria, Rodríguez Nieto Mª Jesús, Ruiz-Hornillos Francisco J, Seijo Maceiras Luis, Robles Barrena Ignacio, Mena-de-Cea Alvaro, Meijide-Míguez Héctor, Sánchez-Pernaute Olga
Fundación Jiménez Díaz (FJD) University Hospital, FJD Health Research Institute, Universidad Autónoma de Madrid (IIS-FJD, UAM), 28040 Madrid, Spain.
Cabueñes Hospital, 33394 Asturias, Spain.
J Clin Med. 2024 Sep 4;13(17):5242. doi: 10.3390/jcm13175242.
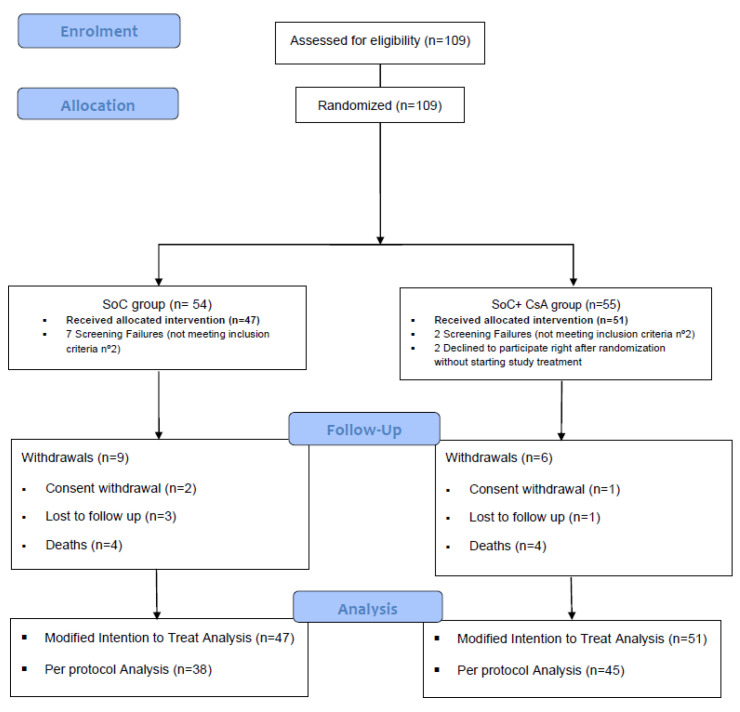
: In susceptible hosts, SARS-CoV2-induced hyperinflammation accounts for an increased mortality. The search of adjuvant immunomodulatory therapies has been ongoing ever since the pandemic outbreak. Aim: Our purpose was to evaluate the efficacy of cyclosporin A (CsA) as an add-on therapy to the standard of care (SoC) in patients with severe COVID-19 pneumonia. : We conducted a randomized clinical trial in patients admitted to eight Spanish tertiary hospitals. Patients were stratified into two severity categories and randomized in a 1:1 ratio to receive a corticosteroid-based standard therapy with or without CsA. The primary endpoint was FiO2 recovery by Day 12 without relapses. : 109 patients were included and randomized, and 98 of them considered for the mITT population (51 assigned to the CsA + SoC group and 47 to the SoC group). A total of 35 (68.6%) patients from the CsA + SoC group and 32 (71.1%) patients from the SoC group reached the primary endpoint in the mITT analysis. No differences were found after stratification into age groups, in the severity level at admission, or in a combination of both. Overall, the time to FiO2 normalization was 7.4 days vs. 7.9 days in the experimental and control groups, respectively. Global mortality was 8.2%. Severe adverse events were uncommon and equally distributed between arms. : The addition of CsA did not show differences over a corticosteroid-based treatment in the clinical course of the included patients. A better identification of candidates who will benefit from receiving immunomodulatory drugs is necessary in future studies.
在易感宿主中,SARS-CoV2 诱导的过度炎症导致死亡率增加。自疫情爆发以来,一直在寻找辅助免疫调节疗法。目的:我们的目的是评估环孢素 A(CsA)作为重度 COVID-19 肺炎患者标准治疗(SoC)附加疗法的疗效。我们在八家西班牙三级医院收治的患者中进行了一项随机临床试验。患者被分为两个严重程度类别,并以 1:1 的比例随机接受基于皮质类固醇的标准治疗,加或不加 CsA。主要终点是第 12 天 FiO2 恢复且无复发。109 名患者被纳入并随机分组,其中 98 名被纳入意向性分析人群(51 名分配到 CsA + SoC 组,47 名分配到 SoC 组)。在 mITT 分析中,CsA + SoC 组共有 35 名(68.6%)患者和 SoC 组 32 名(71.1%)患者达到主要终点。在按年龄组分层、入院时的严重程度水平或两者结合方面均未发现差异。总体而言,实验组和对照组 FiO2 恢复正常的时间分别为 7.4 天和 7.9 天。总死亡率为 8.2%。严重不良事件不常见,且两组分布均匀。在纳入患者的临床过程中,添加 CsA 与基于皮质类固醇的治疗相比没有显示出差异。未来的研究有必要更好地识别将从接受免疫调节药物中获益的候选者。