Division of Population Health and Genomics, University of Dundee, Dundee, UK.
School of Informatics, University of Edinburgh, Edinburgh, UK.
BMC Cardiovasc Disord. 2023 Apr 15;23(1):194. doi: 10.1186/s12872-023-03209-8.
Prediction of lifetime cardiovascular disease (CVD) risk is recommended in many clinical guidelines, but lifetime risk models are rarely externally validated. The aim of this study was to externally validate the QRiskLifetime incident CVD risk prediction tool.
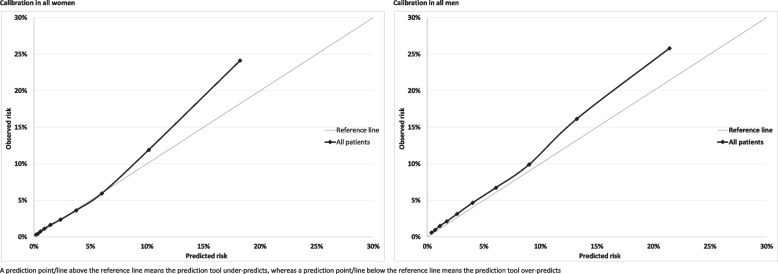
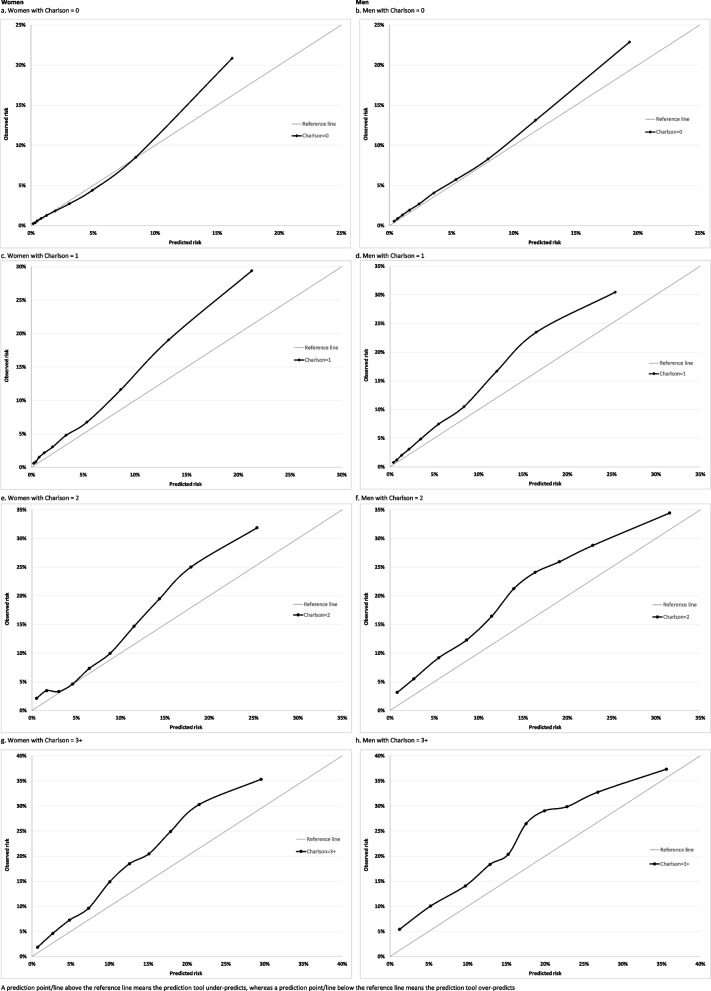
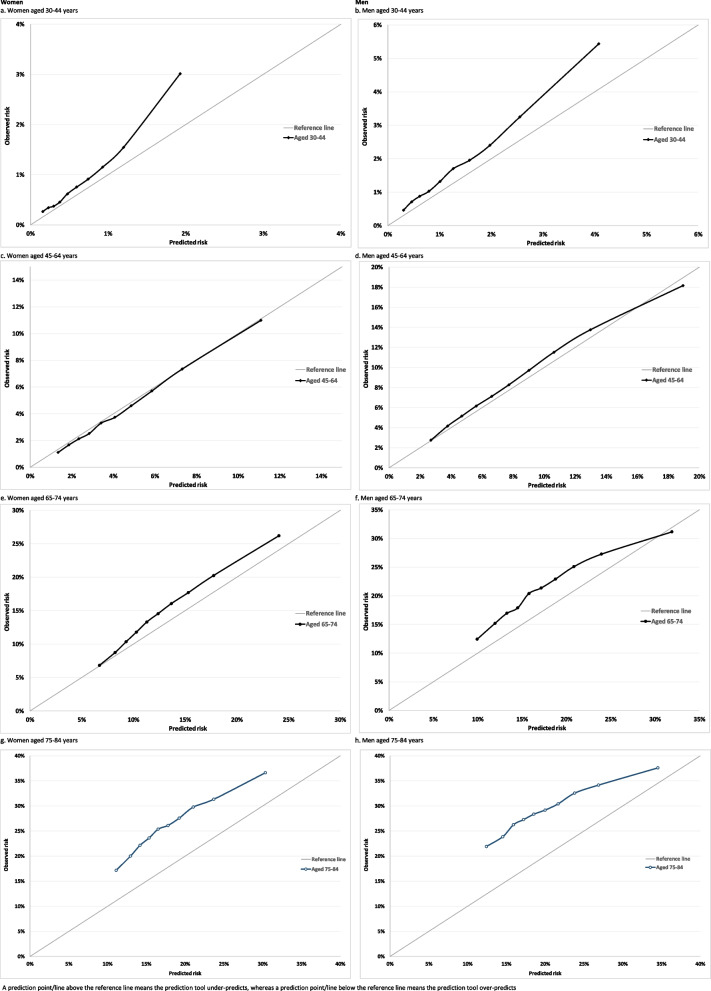
Independent external validation of QRiskLifetime using Clinical Practice Research Datalink data, examining discrimination and calibration in the whole population and stratified by age, and reclassification compared to QRISK3. Since lifetime CVD risk is unobservable, performance was evaluated at 10-years' follow-up, and lifetime performance inferred in terms of performance for in the different age-groups from which lifetime predictions are derived.
One million, two hundreds sixty thousand and three hundreds twenty nine women and 1,223,265 men were included in the analysis. Discrimination was excellent in the whole population (Harrell's-C = 0.844 in women, 0.808 in men), but moderate to poor stratified by age-group (Harrell's C in people aged 30-44 0.714 for both men and women, in people aged 75-84 0.578 in women and 0.556 in men). Ten-year CVD risk was under-predicted in the whole population, and in all age-groups except women aged 45-64, with worse under-prediction in older age-groups. Compared to those at highest QRISK3 estimated 10-year risk, those with highest lifetime risk were younger (mean age: women 50.5 vs. 71.3 years; men 46.3 vs. 63.8 years) and had lower systolic blood pressure and prevalence of treated hypertension, but had more family history of premature CVD, and were more commonly minority ethnic. Over 10-years, the estimated number needed to treat (NNT) with a statin to prevent one CVD event in people with QRISK3 ≥ 10% was 34 in women and 37 in men, compared to 99 and 100 for those at highest lifetime risk.
QRiskLifetime underpredicts 10-year CVD risk in nearly all age-groups, so is likely to also underpredict lifetime risk. Treatment based on lifetime risk has considerably lower medium-term benefit than treatment based on 10-year risk.
许多临床指南建议预测终生心血管疾病(CVD)风险,但终生风险模型很少得到外部验证。本研究旨在对外验证 QRiskLifetime 发生 CVD 风险预测工具。
使用临床实践研究数据链接数据对 QRiskLifetime 进行独立的外部验证,在整个人群中以及按年龄分层检查区分度和校准,并与 QRISK3 进行重新分类比较。由于终生 CVD 风险是不可观察的,因此在 10 年随访时评估其性能,并根据不同年龄组的终生预测推断出不同年龄组的终生性能。
共有 126 万 2653 名女性和 122 万 329 名男性纳入分析。在整个人群中,区分度非常好(女性 Harrell 的 C 值为 0.844,男性为 0.808),但按年龄组分层时为中等至较差(30-44 岁人群的 Harrell 的 C 值为 0.714,男女均为 75-84 岁人群为 0.578,男性为 0.556)。在整个人群中,10 年 CVD 风险被低估,除了 45-64 岁的女性以外,所有年龄组均被低估,在年龄较大的年龄组中,低估情况更为严重。与那些具有最高 QRISK3 估计 10 年风险的人相比,那些具有最高终生风险的人更年轻(女性的平均年龄为 50.5 岁,男性为 63.8 岁),收缩压较低,且患有高血压的比例较低,但患有早发性 CVD 的家族史更多,更常见的是少数民族。在 10 年内,在 QRISK3≥10%的人群中,使用他汀类药物预防 1 例 CVD 事件的估计人数需要治疗(NNT)为女性 34 例,男性 37 例,而终生风险最高的人群为 99 例和 100 例。
QRiskLifetime 在几乎所有年龄组中都低估了 10 年 CVD 风险,因此也可能低估了终生风险。基于终生风险的治疗比基于 10 年风险的治疗具有明显较低的中期获益。