Larsen Tim, Bosworth Matthew L, Ayoubkhani Daniel, Schofield Ryan, Ali Raghib, Khunti Kamlesh, Walker Ann Sarah, Glickman Myer, Harrison Camille, Nafilyan Vahé
Office for National Statistics, Newport, UK.
MRC Epidemiology Unit, Cambridge, UK.
BMJ Med. 2023 Feb 27;2(1):e000187. doi: 10.1136/bmjmed-2022-000187. eCollection 2023.
To examine sociodemographic inequalities in people with SARS-CoV-2 during the second (alpha) and third (delta) waves of the covid-19 pandemic.
Retrospective, population based cohort study.
Resident population of England.
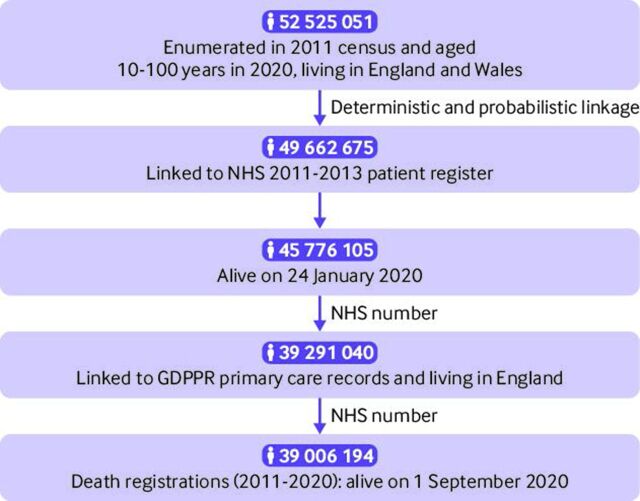
39 006 194 people aged 10 years and older who were enumerated in the 2011 census, registered with the NHS, and alive on 1 September 2020.
Age standardised SARS-CoV-2 case rates (ie, the number of people who received a positive test result per 100 000 person weeks at risk) during the second wave (1 September 2020 to 22 May 2021) or third wave (23 May to 10 December 2021) of the pandemic. Age standardised rates were calculated by sociodemographic characteristics and adjusted rate ratios were estimated using generalised linear regression models with a Poisson distribution (models were adjusted for covariates including sex, age, geographical variables, and sociodemographic characteristics).
During the study period, 5 767 584 people (14.8% of the study population) tested positive for SARS-CoV-2. In the second wave, the fully adjusted relative risks of having a positive test were highest for the Bangladeshi and Pakistani ethnic groups compared with the white British group, with rate ratios of 1.75 (95% confidence interval 1.73 to 1.77) and 1.69 (1.68 to 1.70), respectively. Muslim and Sikh religious groups had fully adjusted rate ratios of 1.51 (1.50 to 1.51) and 1.64 (1.63 to 1.66), respectively, compared with the Christian group. Greater area deprivation, disadvantaged socioeconomic position, living in a care home, and low English language proficiency were also associated with higher relative risk of having a positive test. However, the inequalities among groups varied over time. Being Christian, white British, without a disability, and from a more advantaged socioeconomic position were associated with increased relative risk of testing positive during the third wave.
Research is urgently needed to understand the large sociodemographic inequalities in SARS-CoV-2 case rates in order to inform policy interventions in future waves or pandemics.
研究2019年冠状病毒病(COVID-19)大流行第二波(阿尔法毒株)和第三波(德尔塔毒株)期间感染严重急性呼吸综合征冠状病毒2(SARS-CoV-2)人群的社会人口统计学不平等情况。
基于人群的回顾性队列研究。
英格兰常住人口。
2011年人口普查中登记的、在英国国家医疗服务体系(NHS)注册且于2020年9月1日仍在世的39006194名10岁及以上人群。
大流行第二波(2020年9月1日至2021年5月22日)或第三波(2021年5月23日至12月10日)期间年龄标准化的SARS-CoV-2发病率(即每100000人周的风险中检测呈阳性的人数)。年龄标准化发病率按社会人口统计学特征计算,并使用泊松分布的广义线性回归模型估计调整后的发病率比(模型针对包括性别、年龄、地理变量和社会人口统计学特征在内的协变量进行了调整)。
在研究期间,5767584人(占研究人群的14.8%)SARS-CoV-2检测呈阳性。在第二波疫情中,与英国白人组相比,孟加拉族和巴基斯坦族的完全调整后检测呈阳性的相对风险最高,发病率比分别为1.75(95%置信区间1.73至1.77)和1.69(1.68至1.70)。与基督教组相比,穆斯林和锡克教宗教群体的完全调整后发病率比分别为1.51(1.50至1.51)和1.64(1.63至1.66)。更大程度的地区贫困、社会经济地位不利、住在养老院以及英语水平低也与检测呈阳性的较高相对风险相关。然而,不同群体之间的不平等情况随时间而变化。基督教徒、英国白人、无残疾且社会经济地位更优越的人群在第三波疫情期间检测呈阳性的相对风险增加。
迫切需要开展研究以了解SARS-CoV-2发病率方面巨大的社会人口统计学不平等情况,为未来疫情波次或大流行中的政策干预提供依据。