Maltz-Matyschsyk Michele, Melchiorre Clare K, Herbst Katherine W, Hogan Alexander H, Dibble Kristina, O'Sullivan Brandon, Graf Joerg, Jadhav Aishwarya, Lawrence David A, Lee William T, Carson Kyle J, Radolf Justin D, Salazar Juan C, Lynes Michael A
Department of Molecular and Cell Biology, University of Connecticut, Storrs, CT, United States.
Connecticut Children's Medical Center, Hartford, CT, United States.
Front Bioeng Biotechnol. 2023 Mar 31;11:1066391. doi: 10.3389/fbioe.2023.1066391. eCollection 2023.
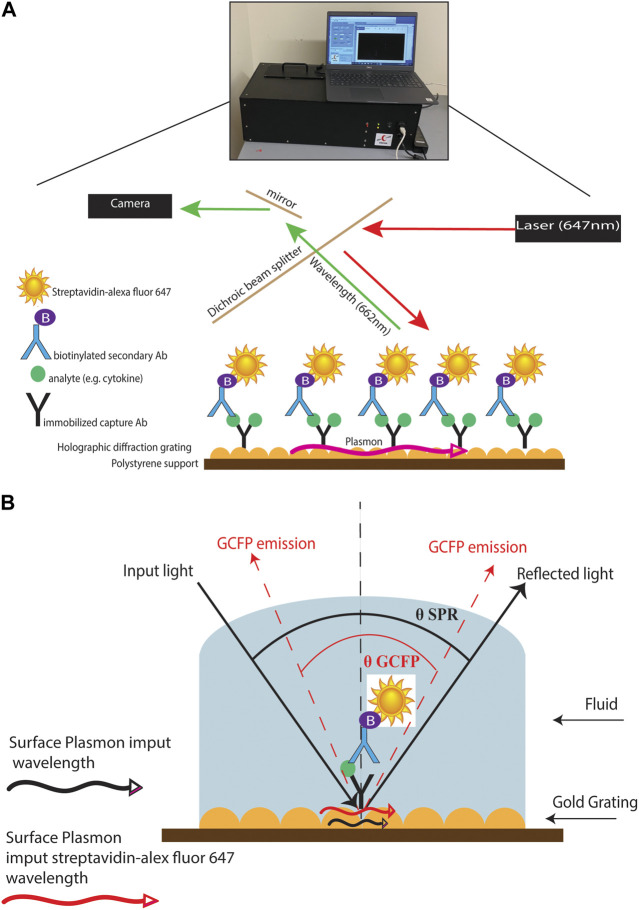
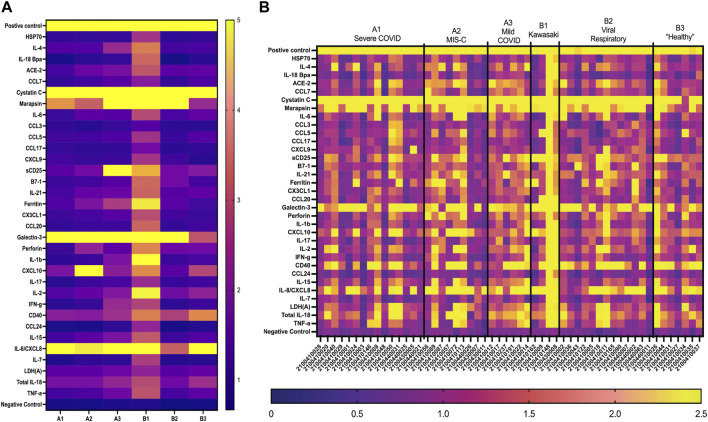
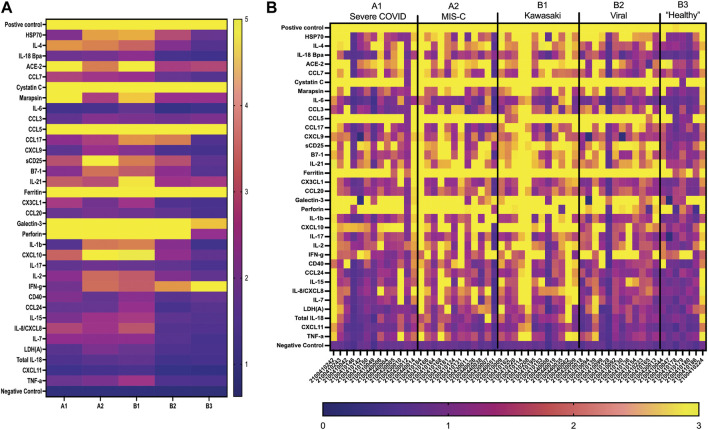
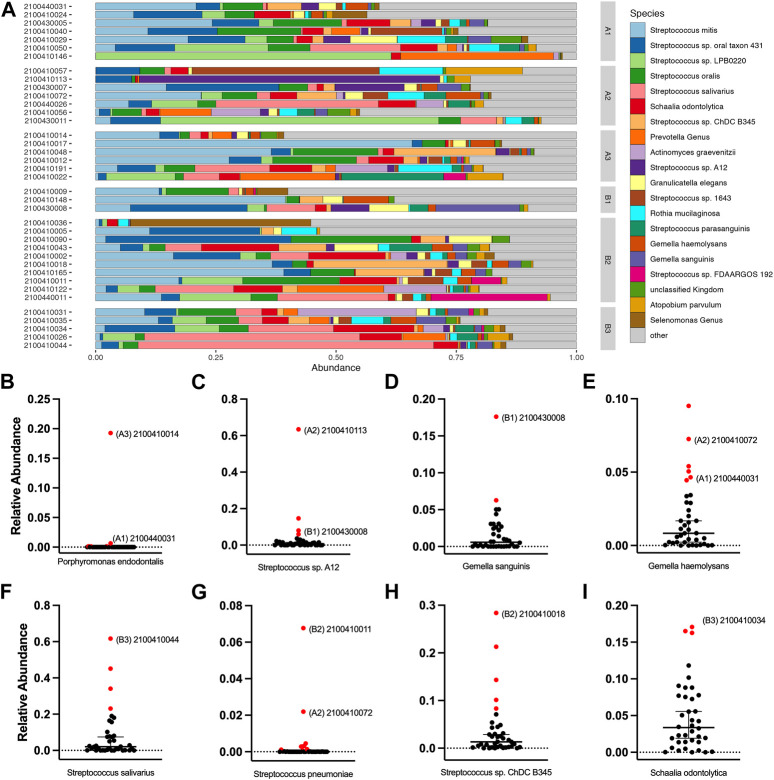
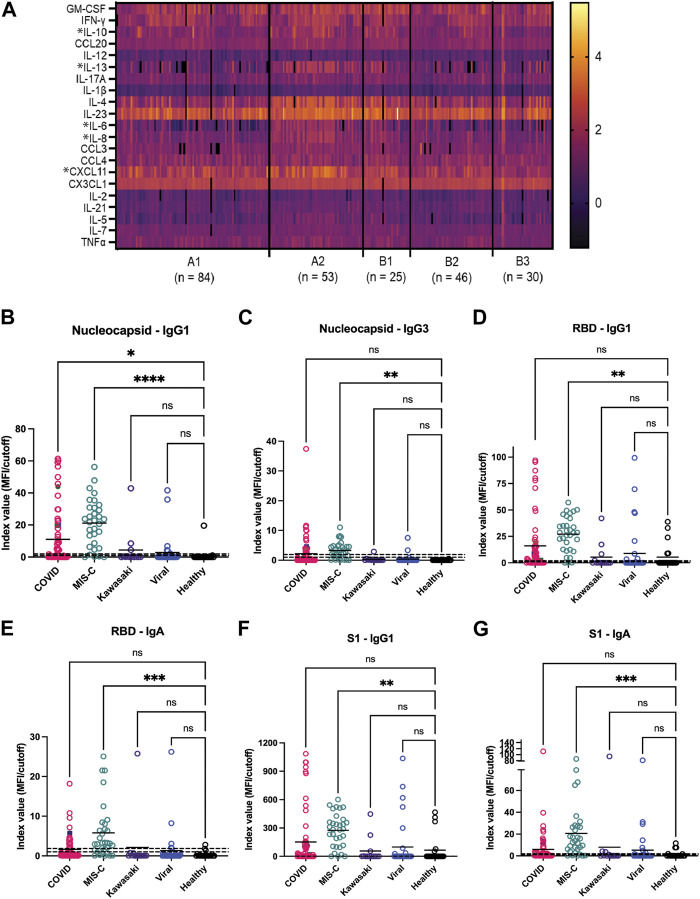
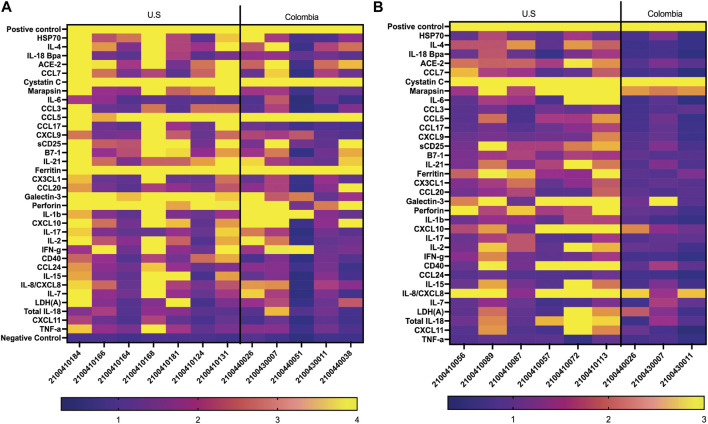
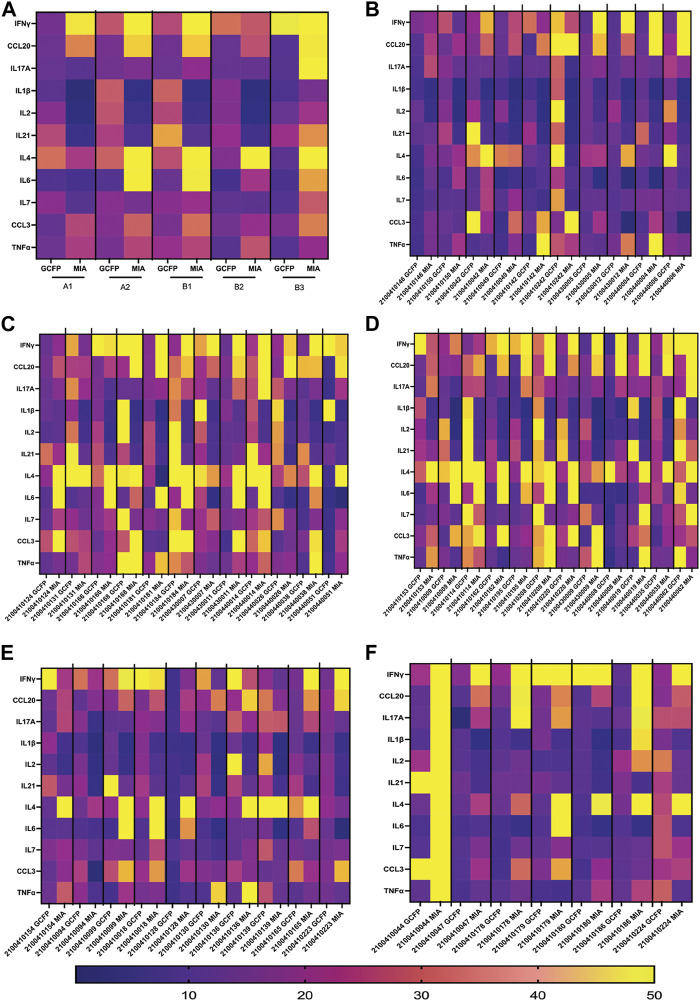
Multisystem inflammatory syndrome in children (MIS-C) is a rare but serious condition that can develop 4-6 weeks after a school age child becomes infected by SARS-CoV-2. To date, in the United States more than 8,862 cases of MIS-C have been identified and 72 deaths have occurred. This syndrome typically affects children between the ages of 5-13; 57% are Hispanic/Latino/Black/non-Hispanic, 61% of patients are males and 100% have either tested positive for SARS-CoV-2 or had direct contact with someone with COVID-19. Unfortunately, diagnosis of MIS-C is difficult, and delayed diagnosis can lead to cardiogenic shock, intensive care admission, and prolonged hospitalization. There is no validated biomarker for the rapid diagnosis of MIS-C. In this study, we used Grating-coupled Fluorescence Plasmonic (GCFP) microarray technology to develop biomarker signatures in pediatric salvia and serum samples from patients with MIS-C in the United States and Colombia. GCFP measures antibody-antigen interactions at individual regions of interest (ROIs) on a gold-coated diffraction grating sensor chip in a sandwich immunoassay to generate a fluorescent signal based on analyte presence within a sample. Using a microarray printer, we designed a first-generation biosensor chip with the capability of capturing 33 different analytes from 80 of sample (saliva or serum). Here, we show potential biomarker signatures in both saliva and serum samples in six patient cohorts. In saliva samples, we noted occasional analyte outliers on the chip within individual samples and were able to compare those samples to 16S RNA microbiome data. These comparisons indicate differences in relative abundance of oral pathogens within those patients. Microsphere Immunoassay (MIA) of immunoglobulin isotypes was also performed on serum samples and revealed MIS-C patients had several COVID antigen-specific immunoglobulins that were significantly higher than other cohorts, thus identifying potential new targets for the second-generation biosensor chip. MIA also identified additional biomarkers for our second-generation chip, verified biomarker signatures generated on the first-generation chip, and aided in second-generation chip optimization. Interestingly, MIS-C samples from the United States had a more diverse and robust signature than the Colombian samples, which was also illustrated in the MIA cytokine data. These observations identify new MIS-C biomarkers and biomarker signatures for each of the cohorts. Ultimately, these tools may represent a potential diagnostic tool for use in the rapid identification of MIS-C.
儿童多系统炎症综合征(MIS-C)是一种罕见但严重的病症,可在学龄儿童感染SARS-CoV-2后4至6周出现。截至目前,美国已确诊8862多例MIS-C病例,并有72例死亡。该综合征通常影响5至13岁的儿童;57%为西班牙裔/拉丁裔/黑人/非西班牙裔,61%的患者为男性,100%的患者SARS-CoV-2检测呈阳性或曾与COVID-19患者有过直接接触。不幸的是,MIS-C的诊断困难,延迟诊断可导致心源性休克、入住重症监护病房和延长住院时间。目前尚无用于快速诊断MIS-C的经过验证的生物标志物。在本研究中,我们使用光栅耦合荧光等离子体(GCFP)微阵列技术,在美国和哥伦比亚MIS-C患者的儿科唾液和血清样本中开发生物标志物特征。GCFP在夹心免疫测定中,于金涂层衍射光栅传感器芯片上的各个感兴趣区域(ROI)测量抗体 - 抗原相互作用,以根据样本中分析物的存在产生荧光信号。使用微阵列打印机,我们设计了一种第一代生物传感器芯片,能够从80微升样本(唾液或血清)中捕获33种不同的分析物。在此,我们展示了六个患者队列的唾液和血清样本中的潜在生物标志物特征。在唾液样本中,我们注意到单个样本芯片上偶尔存在分析物异常值,并能够将这些样本与16S RNA微生物组数据进行比较。这些比较表明这些患者口腔病原体相对丰度的差异。还对血清样本进行了免疫球蛋白同种型的微球免疫测定(MIA),结果显示MIS-C患者有几种COVID抗原特异性免疫球蛋白明显高于其他队列,从而确定了第二代生物传感器芯片的潜在新靶点。MIA还为我们的第二代芯片鉴定了其他生物标志物,验证了在第一代芯片上产生的生物标志物特征,并有助于第二代芯片的优化。有趣的是,来自美国的MIS-C样本比哥伦比亚样本具有更多样化和更强健的特征,这也在MIA细胞因子数据中得到体现。这些观察结果为每个队列确定了新的MIS-C生物标志物和生物标志物特征。最终,这些工具可能代表一种用于快速识别MIS-C的潜在诊断工具。