Noda Mitsuaki, Takahara Shunsuke, Inui Atsuyuki, Oe Keisuke, Osawa Shin, Matsushita Takehiko
Department of Orthopaedics, Nishi Hospital, Kobe, JPN.
Department of Orthopaedics, Hyogo Prefectural Kakogawa Medical Center, Kakogawa, JPN.
Cureus. 2023 Mar 13;15(3):e36103. doi: 10.7759/cureus.36103. eCollection 2023 Mar.
Introduction In a preliminary study of cephalo-medullary (CM) nailing in patients with femoral intertrochanteric fractures, the authors of this study found a 25% to 30% decrease in muscle strength, especially abduction force, during the postoperative follow-up period. This decline was partially attributed to the entry point for the nail insertion causing damage to the gluteus medius tendon at the junction of the greater trochanter after reaming. Therefore, we assumed that changing the position of nail insertion to a "bald spot (BS)" could mitigate postoperative functional impairment. Automated computed tomography (CT) imaging of skeletal muscle cross-sectional area (CSA) and adipose tissue ratio (ATR) can show pathological changes on the operated side compared with the non-operated side. In this study, the authors quantified the difference in postoperative CSA and ATR of the gluteus medius muscle after bald spot nailing versus nail insertion through the conventional tip of the greater trochanter. It was hypothesized that bald spot nailing could avoid significant injury to the gluteus medius muscle. Materials and methods Patients with femoral intertrochanteric fractures were grouped according to the site of cephalo-medullary nailing: greater trochanteric tip (TIP) in 27 patients (8 men and 19 women, mean age 84.9±5.1 years) and BS in 16 patients (3 men and 13 women, mean age 86.9±6.2 years). The CSA and ATR of the gluteus medius muscles were assessed in three slices (A, B, and C from proximal to distal). Each slice was manually traced and automatically calculated based on its contour. Adipose tissue (-100 to -50 in Hounsfield units) in the designated area was distinguished by a bimodal image histogram resulting from the distribution of CT numbers of adipose tissue and muscle. The body mass index (BMI) was used to correct the CSA in each patient. Results In the TIP group, the mean CSA values (mm) from the non-operated/operated sides were as follows: slice A, 2180.2 ± 616.5/1976.3 ± 421.2; slice B, 2112.3 ± 535.7/1857.7 ± 386.7; and slice C: 1671.8 ± 460.0/1404.1 ± 404.3 (p<0.01 in slices A, B, and C). In the BS group, slice A was 2044.1 ± 473.0/2016.9 ± 388.4; slice B was 2073.2 ± 540.7/1848.3 ± 411.1; and slice C was 1659.1 ± 477.2/1468.5 ± 341.7 (p=0.34 in slice A, and p<0.05 in slices B and C, respectively). The mean CSA values (mm) of the non-operated minus operated side between the TIP/BS groups were as follows: slice A, 241.3 ± 424.3/-11.8 ± 285.6; slice B, 290.3 ± 313.0/211.8 ± 333.2; and slice C, 276.4 ± 270.4/162.8 ± 319.3 (p < 0.05 in slice A, 0.45, 0.24 in slices B, C, respectively). The mean adjusted CSA per BMI values (mm) of the non-operated minus the operated side between the TIP/BS groups were slice A, 10.6 ± 19.7/-0.4 ± 14.8; slice B, 13.3 ± 15.0/10.1 ± 16.3; and slice C, 13.1 ± 13.4/ 8.7 ± 15.3 (p < 0.05 in slice A and 0.54 and 0.36 in slices B and C, respectively). Conclusion Nail insertion at the bald spot resulted in a significantly smaller decrease in the CSA of the gluteus medius muscle compared with the conventional tip entry. In addition, an examination of BMI-adjusted CSA showed that CSA was maintained in some image slices. These results suggest that nailing from the BS of the greater trochanter can reduce damage to the gluteus medius muscle and highlight the importance of imaging beyond the usual assessment of skeletal changes.

引言 在一项针对股骨转子间骨折患者的股骨近端髓内钉(CM)固定的初步研究中,本研究的作者发现在术后随访期间肌肉力量,尤其是外展力下降了25%至30%。这种下降部分归因于扩髓后髓内钉插入点对大转子交界处臀中肌腱的损伤。因此,我们推测将髓内钉插入位置改为“无肌点(BS)”可减轻术后功能障碍。骨骼肌横截面积(CSA)和脂肪组织比率(ATR)的自动计算机断层扫描(CT)成像可以显示手术侧与非手术侧相比的病理变化。在本研究中,作者量化了无肌点入钉与通过大转子传统尖端入钉后臀中肌术后CSA和ATR的差异。假设无肌点入钉可以避免对臀中肌造成重大损伤。
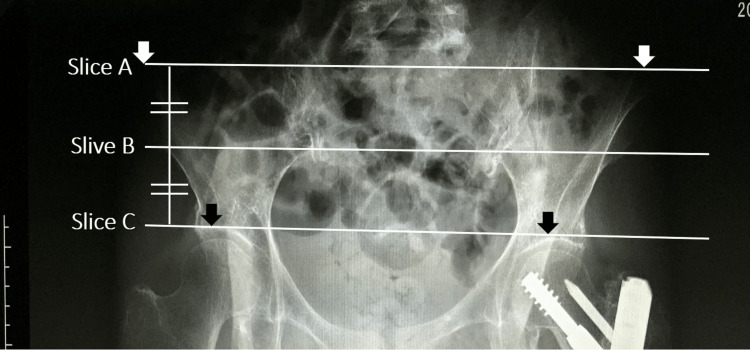
材料与方法 将股骨转子间骨折患者根据股骨近端髓内钉固定部位进行分组:大转子尖端(TIP)组27例(男性8例,女性19例,平均年龄84.9±5.1岁),无肌点(BS)组16例(男性3例,女性13例,平均年龄86.9±6.2岁)。在三个层面(从近端到远端分别为A、B和C)评估臀中肌的CSA和ATR。每个层面均手动勾勒轮廓并根据其轮廓自动计算。通过脂肪组织和肌肉CT值分布产生的双峰图像直方图区分指定区域内的脂肪组织(亨氏单位为-100至-50)。使用体重指数(BMI)对每位患者的CSA进行校正。
结果 在TIP组中,非手术侧/手术侧的平均CSA值(mm)如下:A层面,2180.2±616.5/1976.3±421.2;B层面,2112.3±535.7/1857.7±386.7;C层面:1671.8±460.0/1404.1±404.3(A、B和C层面p<0.01)。在BS组中,A层面为2044.1±473.0/2016.9±388.4;B层面为2073.2±540.7/1848.3±411.1;C层面为1659.1±477.2/1468.5±341.7(A层面p=0.34,B和C层面分别p<0.05)。TIP/BS组之间非手术侧减去手术侧的平均CSA值(mm)如下:A层面,241.3±424.3/-11.8±285.6;B层面,290.3±313.0/211.8±333.2;C层面,276.4±270.4/162.8±319.3(A层面p<0.05,B、C层面分别为0.45、0.24)。TIP/BS组之间非手术侧减去手术侧的每BMI平均校正CSA值(mm)为A层面,10.6±19.7/-0.4±14.8;B层面,13.3±15.0/10.1±16.3;C层面,13.1±13.4/8.7±15.3(A层面p<0.05,B、C层面分别为0.54、0.36)。
结论 与传统尖端入钉相比,在无肌点入钉导致臀中肌CSA的下降明显更小。此外,对BMI校正后的CSA检查显示,在一些图像层面中CSA得以维持。这些结果表明,从大转子无肌点入钉可减少对臀中肌的损伤,并突出了超越骨骼变化常规评估的成像的重要性。