Division of Reproductive Endocrinology and Infertility, Department of Obstetrics and Gynecology, University of Southern California, Los Angeles, California, USA.
Keck School of Medicine, University of Southern California, Los Angeles, California, USA.
Acta Obstet Gynecol Scand. 2023 Jul;102(7):833-842. doi: 10.1111/aogs.14581. Epub 2023 Apr 23.
This study examined obstetric outcomes in patients diagnosed with uterine adenomyosis.
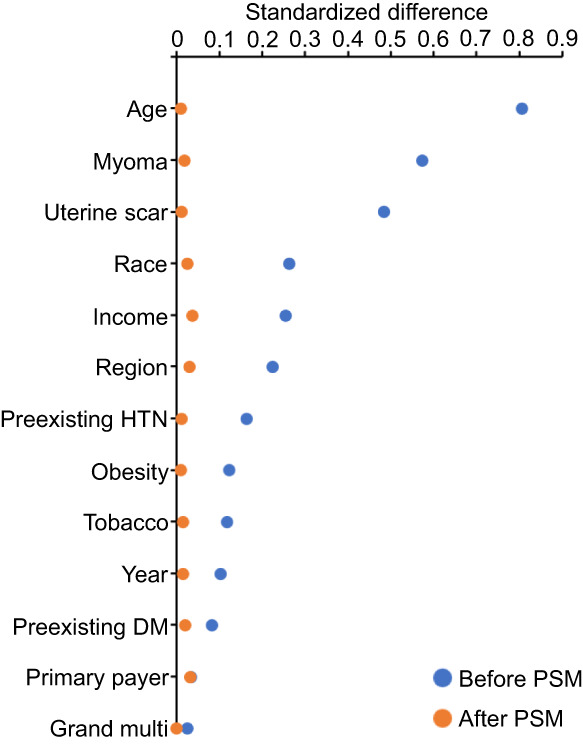
This historical cohort study queried the Healthcare Cost and Utilization Project's National Inpatient Sample. The study population was all hospital deliveries in women aged 15-54 years between January 2016 and December 2019. The exposure was a diagnosis of uterine adenomyosis. The main outcome measures were obstetric characteristics, including placenta previa, placenta accreta spectrum, and placental abruption. Secondary outcomes were delivery complications including severe maternal morbidity. Analytic steps to assess these outcomes included (i) a 1-to-N propensity score matching to mitigate and balance prepregnancy confounders to assess obstetric characteristics, followed by (ii) an adjusting model with preselected pregnancy and delivery factors to assess maternal morbidity. Sensitivity analyses were also performed with restricted cohorts to account for prior uterine scar, uterine myoma, and extra-uterine endometriosis.
After propensity score matching, 5430 patients with adenomyosis were compared to 21 720 patients without adenomyosis. Adenomyosis was associated with an increased odds of placenta accreta spectrum (adjusted-odds ratio [aOR] 3.07, 95% confidence interval [CI] 2.01-4.70), placenta abruption (aOR 3.21, 95% CI: 2.60-3.98), and placenta previa (aOR 5.08, 95% CI: 4.25-6.06). Delivery at <32 weeks of gestation (aOR 1.48, 95% CI: 1.24-1.77) and cesarean delivery (aOR 7.72, 95% CI: 7.04-8.47) were both increased in women with adenomyosis. Patients in the adenomyosis group were more likely to experience severe maternal morbidity at delivery compared to those in the nonadenomyosis group (aOR 1.86, 95% CI: 1.59-2.16). Results remained robust in the aforementioned several sensitivity analyses.
This national-level analysis suggests that a diagnosis of uterine adenomyosis is associated with an increased risk of placental pathology (placenta accreta spectrum, placenta abruption, and placental previa) and adverse maternal outcomes at delivery.
本研究探讨了诊断为子宫腺肌病患者的产科结局。
这是一项历史性队列研究,对医疗保健成本和利用项目的全国住院患者样本进行了查询。研究人群为 2016 年 1 月至 2019 年 12 月期间 15-54 岁的所有医院分娩的女性。暴露因素为子宫腺肌病的诊断。主要结局指标为产科特征,包括前置胎盘、胎盘植入谱系和胎盘早剥。次要结局指标为分娩并发症,包括严重产妇发病率。评估这些结局的分析步骤包括:(i)1 对 N 倾向评分匹配以减轻和平衡孕前混杂因素,以评估产科特征,随后(ii)调整具有预选定妊娠和分娩因素的模型,以评估产妇发病率。还进行了敏感性分析,纳入了限制队列以考虑既往子宫瘢痕、子宫平滑肌瘤和子宫外子宫内膜异位症。
在倾向评分匹配后,将 5430 例腺肌病患者与 21720 例无腺肌病患者进行比较。腺肌病与胎盘植入谱系(调整后的优势比[aOR]3.07,95%置信区间[CI]2.01-4.70)、胎盘早剥(aOR 3.21,95%CI:2.60-3.98)和前置胎盘(aOR 5.08,95%CI:4.25-6.06)的发生几率增加相关。<32 周分娩(aOR 1.48,95%CI:1.24-1.77)和剖宫产分娩(aOR 7.72,95%CI:7.04-8.47)在腺肌病患者中均增加。与非腺肌病组相比,腺肌病组患者在分娩时更有可能出现严重的产妇发病率(aOR 1.86,95%CI:1.59-2.16)。在上述几种敏感性分析中,结果仍然稳健。
这项全国性分析表明,子宫腺肌病的诊断与胎盘病理(胎盘植入谱系、胎盘早剥和前置胎盘)和分娩时不良产妇结局的风险增加相关。