Department of Surgery, Boston University Chobanian and Avedisian School of Medicine, Boston, MA, USA.
Department of Surgery, Boston Medical Center, Boston, MA, USA.
Ann Surg Oncol. 2023 Jul;30(7):4249-4259. doi: 10.1245/s10434-023-13468-6. Epub 2023 Apr 26.
The COVID-19 pandemic strained oncologic care access and delivery, yet little is known about how it impacted hepatocellular carcinoma (HCC) management. Our study sought to evaluate the annual effect of the COVID-19 pandemic on time to treatment initiation (TTI) for HCC.
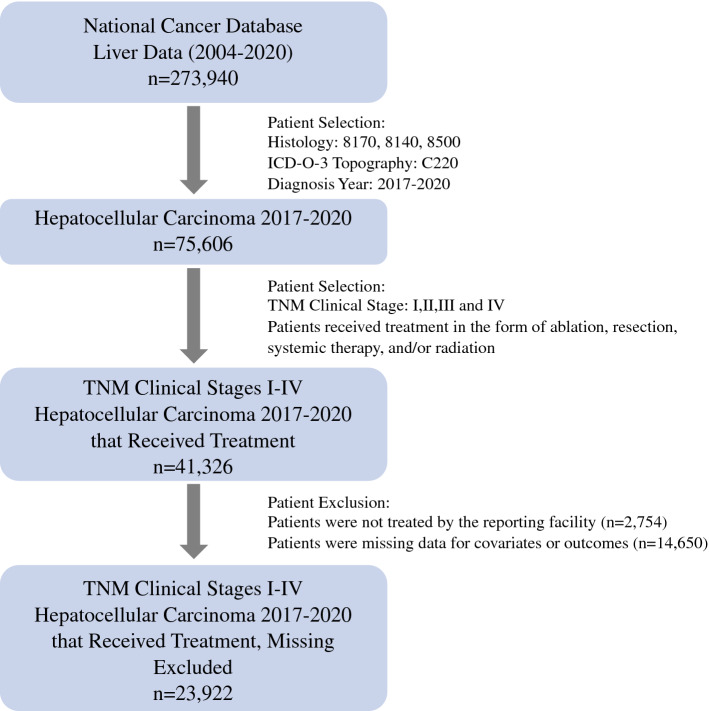
The National Cancer Database was queried for patients diagnosed with clinical stages I-IV HCC (2017-2020). Patients were categorized based on their year of diagnosis as "Pre-COVID" (2017-2019) and "COVID" (2020). TTI based on stage and type of treatment first received was compared by the Mann-Whitney U test. A logistic regression model was used to evaluate factors of increased TTI and treatment delay (> 90 days).
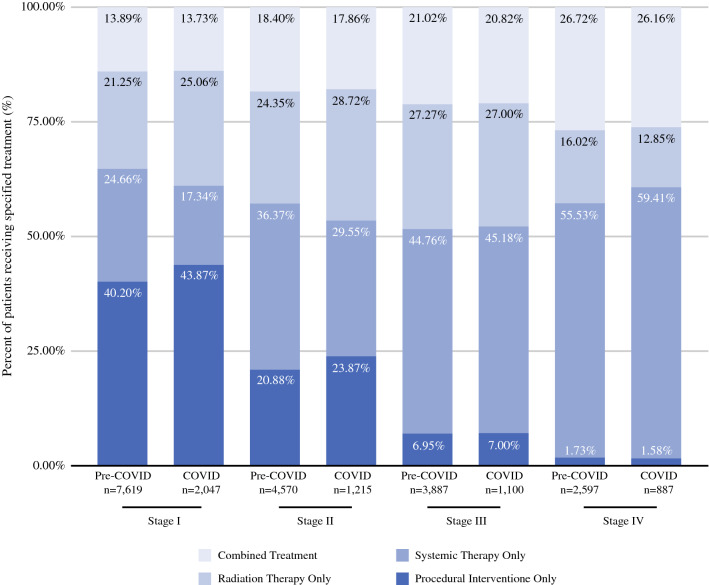
In total, 18,673 patients were diagnosed during Pre-COVID, whereas 5249 were diagnosed during COVID. Median TTI for any first-line treatment modality was slightly shorter during the COVID year compared with Pre-COVID (49 vs. 51 days; p < 0.0001), notably in time to ablation (52 vs. 55 days; p = 0.0238), systemic therapy (42 vs. 47 days; p < 0.0001), and radiation (60 vs. 62 days; p = 0.0177), but not surgery (41 vs. 41 days; p = 0.6887). In a multivariate analysis, patients of Black race, Hispanic ethnicity, and uninsured/Medicaid/Other Government insurance status were associated with increased TTI by factors of 1.057 (95% CI: 1.022-1.093; p = 0.0013), 1.045 (95% CI: 1.010-1.081; p = 0.0104), and 1.088 (95% CI: 1.053-1.123; p < 0.0001), respectively. Similarly, these patient populations were associated with delayed treatment times.
For patients diagnosed during COVID, TTI for HCC, while statistically significant, had no clinically significant differences. However, vulnerable patients were more likely to have increased TTI.
COVID-19 大流行影响了肿瘤治疗的可及性和实施,但其对肝细胞癌(HCC)管理的影响知之甚少。本研究旨在评估 COVID-19 大流行对 HCC 患者治疗起始时间(TTI)的年度影响。
本研究通过国家癌症数据库,对 2017 年至 2020 年间诊断为临床分期 I-IV 期 HCC 的患者进行了检索。患者根据诊断年份分为“大流行前”(2017-2019 年)和“COVID”(2020 年)两组。采用 Mann-Whitney U 检验比较了不同分期和首次治疗类型的 TTI。采用 logistic 回归模型评估了 TTI 延长和治疗延迟(>90 天)的相关因素。
共纳入 18673 例大流行前诊断的患者和 5249 例 COVID 期间诊断的患者。与大流行前相比,COVID 期间任何一线治疗方案的 TTI 均略有缩短(49 天 vs. 51 天;p<0.0001),尤其在消融(52 天 vs. 55 天;p=0.0238)、全身治疗(42 天 vs. 47 天;p<0.0001)和放疗(60 天 vs. 62 天;p=0.0177)方面,而手术治疗的 TTI 无明显差异(41 天 vs. 41 天;p=0.6887)。多因素分析显示,黑种人、西班牙裔、无保险/医疗补助/其他政府保险的患者 TTI 延长的相关因素分别为 1.057(95%CI:1.022-1.093;p=0.0013)、1.045(95%CI:1.010-1.081;p=0.0104)和 1.088(95%CI:1.053-1.123;p<0.0001)。同样,这些患者人群与治疗延迟相关。
对于 COVID 期间诊断的患者,HCC 的 TTI 虽然具有统计学意义,但无临床显著差异。然而,高危患者的 TTI 延长更为明显。