Moon In Tae, Kim Sun-Hwa, Chin Jung Yeon, Park Sung Hun, Yoon Chang-Hwan, Youn Tae-Jin, Chae In-Ho, Kang Si-Hyuck
Uijeongbu Eulji University Hospital, Uijeongbu, Republic of Korea.
Seoul National University Bundang Hospital, Seongnam, Republic of Korea.
JMIR Cardio. 2023 Apr 26;7:e45299. doi: 10.2196/45299.
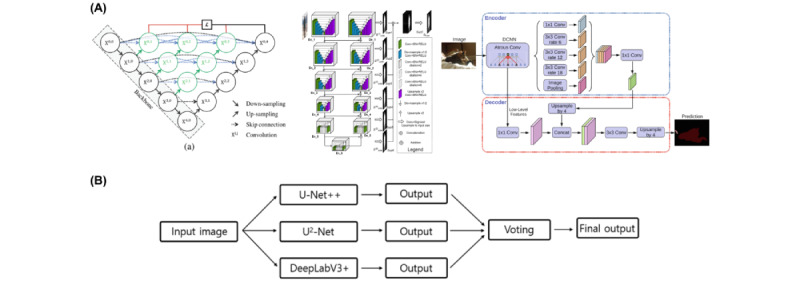
An accurate quantitative analysis of coronary artery stenotic lesions is essential to make optimal clinical decisions. Recent advances in computer vision and machine learning technology have enabled the automated analysis of coronary angiography.
The aim of this paper is to validate the performance of artificial intelligence-based quantitative coronary angiography (AI-QCA) in comparison with that of intravascular ultrasound (IVUS).
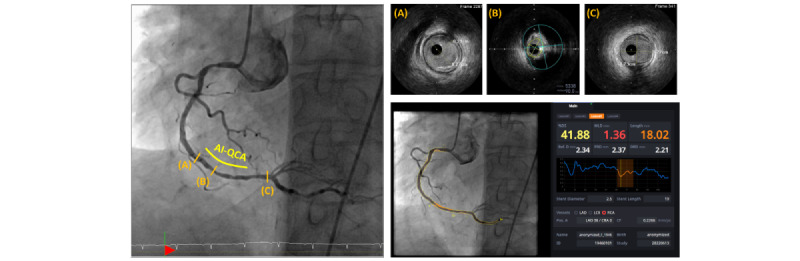
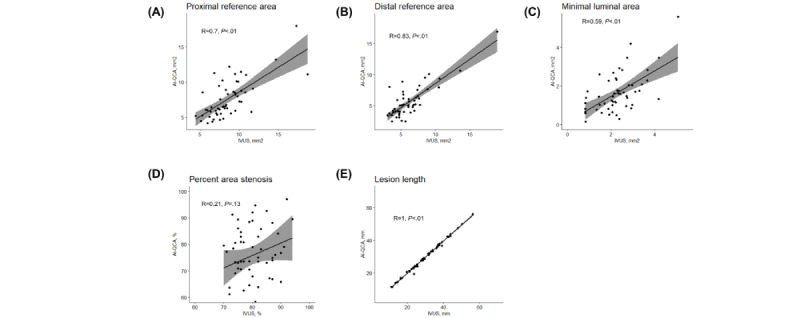
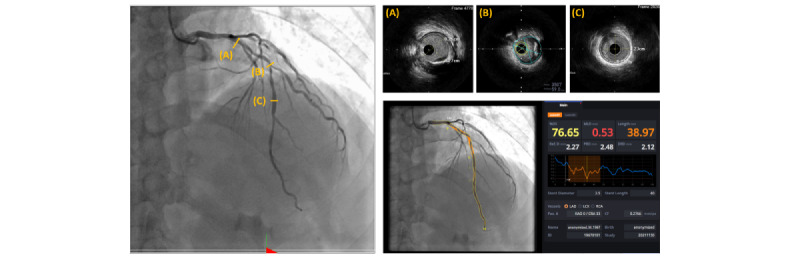
This retrospective study included patients who underwent IVUS-guided coronary intervention at a single tertiary center in Korea. Proximal and distal reference areas, minimal luminal area, percent plaque burden, and lesion length were measured by AI-QCA and human experts using IVUS. First, fully automated QCA analysis was compared with IVUS analysis. Next, we adjusted the proximal and distal margins of AI-QCA to avoid geographic mismatch. Scatter plots, Pearson correlation coefficients, and Bland-Altman were used to analyze the data.
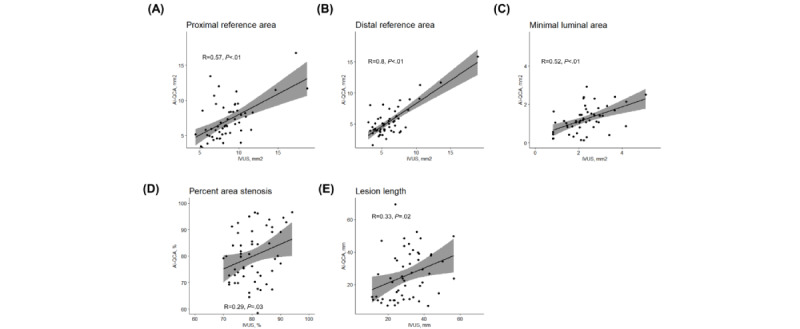
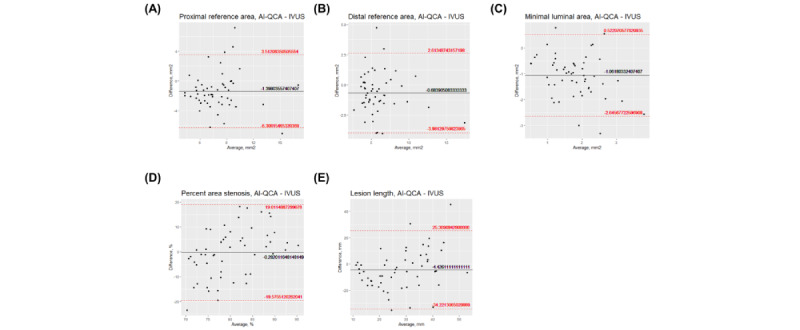
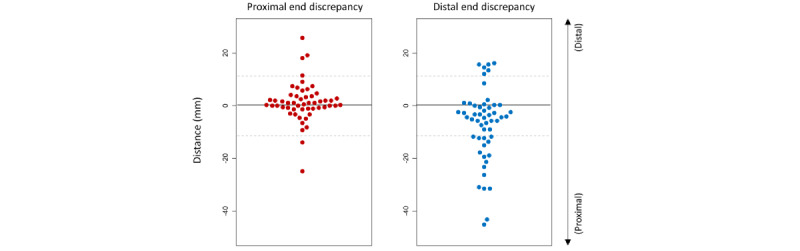
A total of 54 significant lesions were analyzed in 47 patients. The proximal and distal reference areas, as well as the minimal luminal area, showed moderate to strong correlation between the 2 modalities (correlation coefficients of 0.57, 0.80, and 0.52, respectively; P<.001). The correlation was weaker for percent area stenosis and lesion length, although statistically significant (correlation coefficients of 0.29 and 0.33, respectively). AI-QCA tended to measure reference vessel areas smaller and lesion lengths shorter than IVUS did. Systemic proportional bias was not observed in Bland-Altman plots. The biggest cause of bias originated from the geographic mismatch of AI-QCA with IVUS. Discrepancies in the proximal or distal lesion margins were observed between the 2 modalities, which were more frequent at the distal margins. After the adjustment of proximal or distal margins, there was a stronger correlation of proximal and distal reference areas between AI-QCA and IVUS (correlation coefficients of 0.70 and 0.83, respectively).
AI-QCA showed a moderate to strong correlation compared with IVUS in analyzing coronary lesions with significant stenosis. The main discrepancy was in the perception of the distal margins by AI-QCA, and the correction of margins improved the correlation coefficients. We believe that this novel tool could provide confidence to treating physicians and help in making optimal clinical decisions.
对冠状动脉狭窄病变进行准确的定量分析对于做出最佳临床决策至关重要。计算机视觉和机器学习技术的最新进展使得冠状动脉造影的自动分析成为可能。
本文旨在比较基于人工智能的定量冠状动脉造影(AI-QCA)与血管内超声(IVUS)的性能。
这项回顾性研究纳入了在韩国一家三级中心接受IVUS引导下冠状动脉介入治疗的患者。近端和远端参考面积、最小管腔面积、斑块负荷百分比和病变长度由AI-QCA和使用IVUS的人类专家测量。首先,将全自动QCA分析与IVUS分析进行比较。接下来,我们调整了AI-QCA的近端和远端边界以避免地理不匹配。使用散点图、Pearson相关系数和Bland-Altman分析数据。
共分析了47例患者的54处显著病变。近端和远端参考面积以及最小管腔面积在两种方法之间显示出中度至强相关性(相关系数分别为0.57、0.80和0.52;P<0.001)。面积狭窄百分比和病变长度的相关性较弱,尽管具有统计学意义(相关系数分别为0.29和0.33)。与IVUS相比,AI-QCA倾向于测量更小的参考血管面积和更短的病变长度。Bland-Altman图中未观察到系统性比例偏差。偏差的最大原因源于AI-QCA与IVUS的地理不匹配。两种方法在近端或远端病变边界处存在差异,在远端边界处更频繁。调整近端或远端边界后,AI-QCA与IVUS之间近端和远端参考面积的相关性更强(相关系数分别为0.70和0.83)。
在分析有显著狭窄的冠状动脉病变时,与IVUS相比,AI-QCA显示出中度至强相关性。主要差异在于AI-QCA对远端边界的识别,边界校正提高了相关系数。我们认为这种新工具可以为治疗医生提供信心,并有助于做出最佳临床决策。