Department of Head and Neck-Endocrine Oncology, Moffitt Cancer Center, Tampa, Florida, USA.
Office of Community Outreach, Engagement, and Equity, Moffitt Cancer Center, Tampa, Florida, USA.
Cancer Med. 2023 Jun;12(12):13687-13700. doi: 10.1002/cam4.5992. Epub 2023 Apr 28.
National Cancer Institute cancer centers (NCICCs) provide specialized cancer care including precision oncology and clinical treatment trials. While these centers can offer novel therapeutic options, less is known about when patients access these centers or at what timepoint in their disease course they receive specialized care. This is especially important since precision diagnostics and receipt of the optimal therapy upfront can impact patient outcomes and previous research suggests that access to these centers may vary by demographic characteristics. Here, we examine the timing of patients' presentation at Moffitt Cancer Center (MCC) relative to their initial diagnosis across several demographic characteristics.
A retrospective cohort study was conducted among patients who presented to MCC with breast, colon, lung, melanoma, and prostate cancers between December 2008 and April 2020. Patient demographic and clinical characteristics were obtained from the Moffitt Cancer Registry. The association between patient characteristics and the timing of patient presentation to MCC relative to the patient's cancer diagnosis was examined using logistic regression.
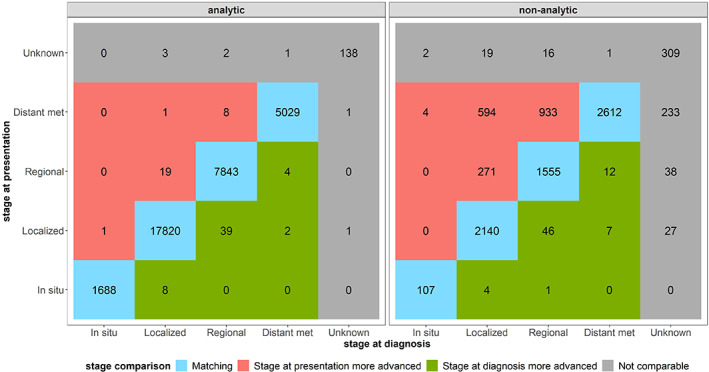
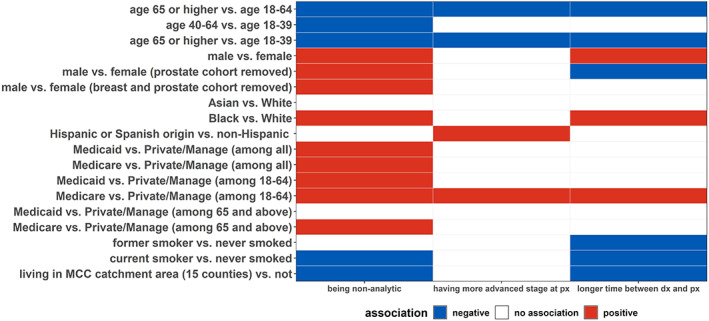
Black patients (median days = 510) had a longer time between diagnosis and presentation to MCC compared to Whites (median days = 368). Black patients were also more likely to have received their initial cancer care outside of MCC compared to White patients (odds ratio [OR] and 95% confidence interval [CI] = 1.45 [1.32-1.60]). Furthermore, Hispanics were more likely to present to MCC at an advanced stage compared to non-Hispanic patients (OR [95% CI] = 1.28 [1.05-1.55]).
We observed racial and ethnic differences in timing of receipt of care at MCC. Future studies should aim to identify contributing factors for the development of novel mitigation strategies and assess whether timing differences in referral to an NCICC correlate with long-term patient outcomes.
美国国家癌症研究所癌症中心(NCICCs)提供专业的癌症治疗,包括精准肿瘤学和临床试验治疗。虽然这些中心可以提供新的治疗选择,但患者何时获得这些中心的治疗或在疾病过程中的何时获得专业治疗知之甚少。这一点非常重要,因为精准诊断和尽早接受最佳治疗可以影响患者的预后,而且之前的研究表明,进入这些中心的机会可能因人口统计学特征而异。在这里,我们研究了患者在莫菲特癌症中心(MCC)就诊的时间与他们在几个人口统计学特征方面的初始诊断的关系。
我们对 2008 年 12 月至 2020 年 4 月期间在 MCC 就诊的患有乳腺癌、结肠癌、肺癌、黑色素瘤和前列腺癌的患者进行了回顾性队列研究。患者的人口统计学和临床特征从莫菲特癌症登记处获得。使用逻辑回归检查患者特征与患者向 MCC 就诊的时间与患者癌症诊断的关系。
与白人患者(中位天数为 368 天)相比,黑人患者(中位天数为 510 天)从诊断到向 MCC 就诊的时间间隔更长。与白人患者相比,黑人患者更有可能在 MCC 以外的地方接受初始癌症治疗(比值比[OR]和 95%置信区间[CI]为 1.45[1.32-1.60])。此外,与非西班牙裔患者相比,西班牙裔患者更有可能在晚期阶段向 MCC 就诊(OR[95%CI]为 1.28[1.05-1.55])。
我们观察到在 MCC 接受治疗的时间上存在种族和民族差异。未来的研究应旨在确定制定新的缓解策略的促成因素,并评估向 NCICC 转诊的时间差异是否与长期患者预后相关。