School of Public Health, San Diego State University, San Diego, California, USA.
Moores Cancer Center, University of California San Diego, La Jolla, California, USA.
Cancer. 2022 Oct 1;128(19):3479-3486. doi: 10.1002/cncr.34404. Epub 2022 Aug 2.
Locally advanced cervical cancer (CC) remains lethal in the United States. We investigate the effect of receiving care at an National Cancer Institute-designated cancer center (NCICC) on survival.
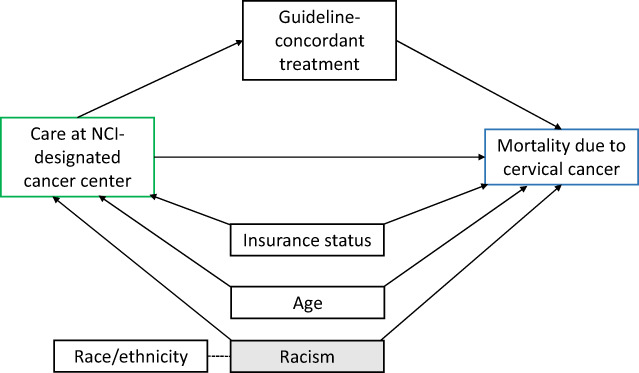
Data for women diagnosed with CC from 2004 to 2016 who received radiation treatment were extracted from the California Cancer Registry (n = 4250). Cox proportional hazards regression models assessed whether (1) receiving care at NCICCs was associated with risk of CC-specific death, (2) this association remained after multivariable adjustment for age, race/ethnicity, and insurance status, and (3) this association was explained by receipt of guideline-concordant treatment.
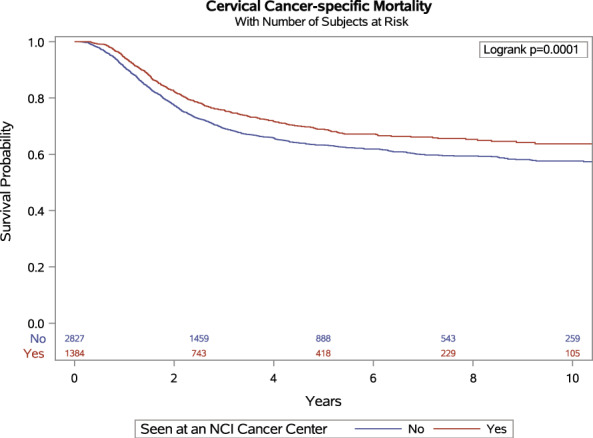
Median age was 50 years (interquartile range [IQR] 41-61 years), with median follow-up of 2.7 years (IQR 1.3-6.0 years). One-third of patients were seen at an NCICC, and 29% died of CC. The hazard of CC-specific death was reduced by 20% for those receiving care at NCICCs compared with patients receiving care elsewhere (HR = .80; 95% CI, 0.70-0.90). Adjustment for guideline-concordant treatment and other covariates minimally attenuated the association to 0.83 (95% CI, 0.74-0.95), suggesting that the survival advantage associated with care at NCICCs may not be due to receipt of guideline-concordant treatment.
This study demonstrates survival benefit for patients receiving care at NCICCs compared with those receiving care elsewhere that is not explained by differences in guideline-concordant care. Structural, organizational, or provider characteristics and differences in patients receiving care at centers with and without NCI designation could explain observed associations. Further understanding of these factors will promote equality across oncology care facilities and survival equity for patients with CC.
在美国,局部晚期宫颈癌(CC)仍然是致命的。我们研究了在被美国国立癌症研究所(NCI)指定的癌症中心(NCICC)接受治疗对生存的影响。
从加利福尼亚癌症登记处(n=4250)提取了 2004 年至 2016 年期间被诊断患有 CC 并接受放射治疗的女性的数据。Cox 比例风险回归模型评估了以下情况:(1)在 NCICCs 接受治疗是否与 CC 特异性死亡风险相关;(2)在对年龄、种族/民族和保险状况进行多变量调整后,这种关联是否仍然存在;(3)这种关联是否可以通过接受符合指南的治疗来解释。
中位年龄为 50 岁(四分位距[IQR] 41-61 岁),中位随访时间为 2.7 年(IQR 1.3-6.0 年)。三分之一的患者在 NCICC 就诊,29%的患者死于 CC。与在其他地方接受治疗的患者相比,在 NCICCs 接受治疗的患者 CC 特异性死亡的风险降低了 20%(HR=0.80;95%CI,0.70-0.90)。调整符合指南的治疗和其他协变量后,相关性最小减弱至 0.83(95%CI,0.74-0.95),这表明与在 NCICCs 接受治疗相关的生存优势可能不是由于接受符合指南的治疗。
与在其他地方接受治疗的患者相比,本研究表明在 NCICCs 接受治疗的患者具有生存优势,而这种优势不能用符合指南的治疗差异来解释。在有和没有 NCI 指定的中心接受治疗的患者之间的结构性、组织性或提供者特征以及差异可能解释了观察到的关联。进一步了解这些因素将促进肿瘤学治疗设施之间的平等,并为 CC 患者实现生存公平。