Hill Joshua A, Martens Michael J, Young Jo-Anne H, Bhavsar Kavita, Kou Jianqun, Chen Min, Lee Lik Wee, Baluch Aliyah, Dhodapkar Madhav V, Nakamura Ryotaro, Peyton Kristin, Shahid Zainab, Armistead Paul, Westervelt Peter, McCarty John, McGuirk Joseph, Hamadani Mehdi, DeWolf Susan, Hosszu Kinga, Sharon Elad, Spahn Ashley, Toor Amir A, Waldvogel Stephanie, Greenberger Lee M, Auletta Jeffery J, Horowitz Mary M, Riches Marcie L, Perales Miguel-Angel
Vaccine and Infectious Disease, Fred Hutchinson Cancer Center, Seattle, WA, USA.
Department of Medicine, University of Washington, Seattle, WA, USA.
EClinicalMedicine. 2023 May;59:101983. doi: 10.1016/j.eclinm.2023.101983. Epub 2023 Apr 27.
The optimal timing for SARS-CoV-2 vaccines within the first year after allogeneic hematopoietic cell transplant (HCT) is poorly understood.
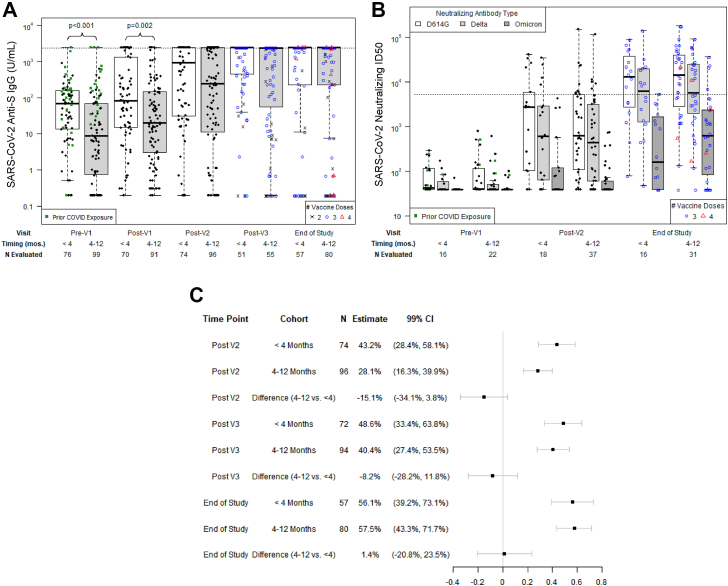
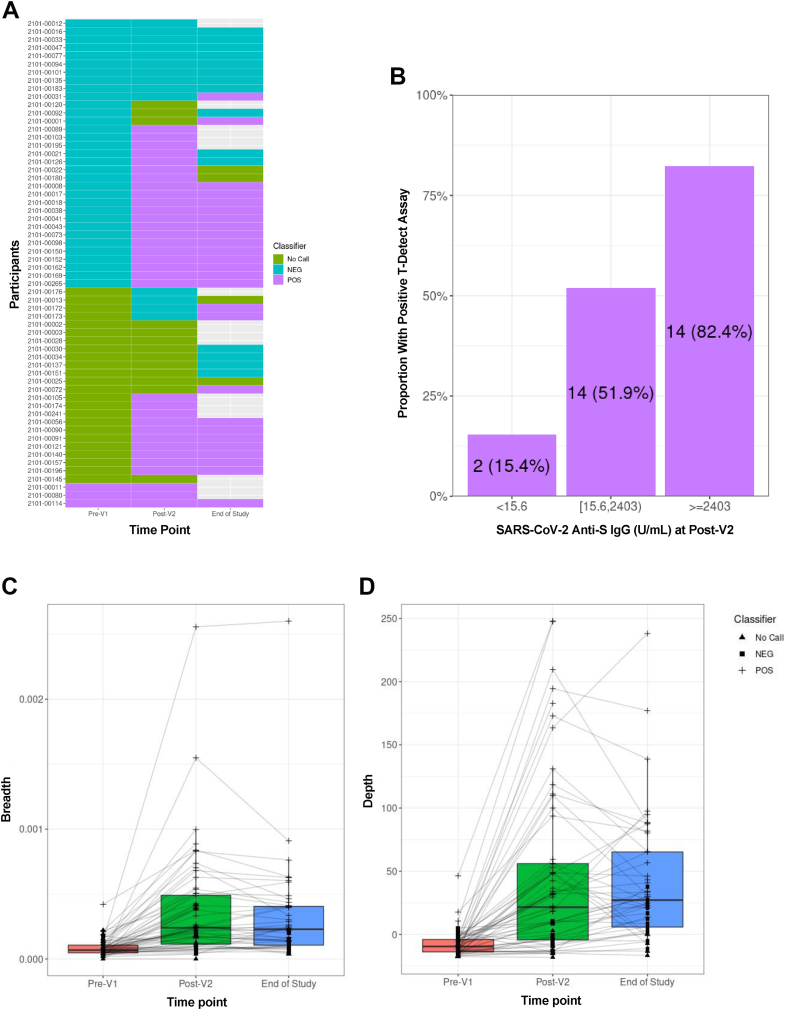
We conducted a prospective, multicentre, observational study of allogeneic HCT recipients who initiated SARS-CoV-2 vaccinations within 12 months of HCT. Participants were enrolled at 22 academic cancer centers across the United States. Participants of any age who were planning to receive a first post-HCT SARS-CoV-2 vaccine within 12 months of HCT were eligible. We obtained blood prior to and after each vaccine dose for up to four vaccine doses, with an end-of-study sample seven to nine months after enrollment. We tested for SARS-CoV-2 spike protein (anti-S) IgG; nucleocapsid protein (anti-N) IgG; neutralizing antibodies for Wuhan D614G, Delta B.1.617.2, and Omicron B.1.1.529 strains; and SARS-CoV-2-specific T-cell receptors (TCRs). The primary outcome was a comparison of anti-S IgG titers at the post-V2 time point in participants initiating vaccinations <4 months versus 4-12 months after HCT using a propensity-adjusted analysis. We also evaluated factors associated with high-level anti-S IgG titers (≥2403 U/mL) in logistic regression models.
Between April 22, 2021 and November 17, 2021, 175 allogeneic HCT recipients were enrolled in the study, of whom all but one received mRNA SARS-CoV-2 vaccines. SARS-CoV-2 anti-S IgG titers, neutralizing antibody titers, and TCR breadth and depth did not significantly differ at all tested time points following the second vaccination among those initiating vaccinations <4 months versus 4-12 months after HCT. Anti-S IgG ≥2403 U/mL correlated with neutralizing antibody levels similar to those observed in a prior study of non-immunocompromised individuals, and 57% of participants achieved anti-S IgG ≥2403 U/mL at the end-of-study time point. In models adjusted for SARS-CoV-2 infection pre-enrollment, SARS-CoV-2 vaccination pre-HCT, CD19+ B-cell count, CD4+ T-cell count, and age (as applicable to the model), vaccine initiation timing was not associated with high-level anti-S IgG titers at the post-V2, post-V3, or end-of-study time points. Notably, prior graft-versus-host-disease (GVHD) or use of immunosuppressive medications were not associated with high-level anti-S IgG titers. Grade ≥3 vaccine-associated adverse events were infrequent.
These data support starting mRNA SARS-CoV-2 vaccination three months after HCT, irrespective of concurrent GVHD or use of immunosuppressive medications. This is one of the largest prospective analyses of vaccination for any pathogen within the first year after allogeneic HCT and supports current guidelines for SARS-CoV-2 vaccination starting three months post-HCT. Additionally, there are few studies of mRNA vaccine formulations for other pathogens in HCT recipients, and these data provide encouraging proof-of-concept for the utility of early vaccination targeting additional pathogens with mRNA vaccine platforms.
National Marrow Donor Program, Leukemia and Lymphoma Society, Multiple Myeloma Research Foundation, Novartis, LabCorp, American Society for Transplantation and Cellular Therapy, Adaptive Biotechnologies, and the National Institutes of Health.
对于异基因造血细胞移植(HCT)后第一年接种严重急性呼吸综合征冠状病毒2(SARS-CoV-2)疫苗的最佳时机,目前了解不足。
我们对在HCT后12个月内开始接种SARS-CoV-2疫苗的异基因HCT受者进行了一项前瞻性、多中心观察性研究。参与者在美国22个学术癌症中心入组。任何年龄且计划在HCT后12个月内接受首剂HCT后SARS-CoV-2疫苗的参与者均符合条件。我们在每次接种疫苗前后采集血液,最多采集四剂疫苗的血样,并在入组后7至9个月采集研究结束时的样本。我们检测了SARS-CoV-2刺突蛋白(抗S)IgG;核衣壳蛋白(抗N)IgG;针对武汉D614G、德尔塔B.1.617.2和奥密克戎B.1.1.529毒株的中和抗体;以及SARS-CoV-2特异性T细胞受体(TCR)。主要结局是通过倾向调整分析比较在HCT后<4个月与4 - 12个月开始接种疫苗的参与者在接种第二剂疫苗后时间点的抗S IgG滴度。我们还在逻辑回归模型中评估了与高水平抗S IgG滴度(≥2403 U/mL)相关的因素。
在2021年4月22日至2021年11月17日期间,175名异基因HCT受者入组本研究,其中除一人外均接种了mRNA SARS-CoV-2疫苗。在HCT后<4个月与4 - 12个月开始接种疫苗的参与者中,第二次接种后所有测试时间点的SARS-CoV-2抗S IgG滴度、中和抗体滴度以及TCR广度和深度均无显著差异。抗S IgG≥2403 U/mL与中和抗体水平相关,类似于在先前一项针对非免疫受损个体的研究中观察到的情况,并且57%的参与者在研究结束时达到抗S IgG≥2403 U/mL。在针对入组前的SARS-CoV-2感染、HCT前的SARS-CoV-2疫苗接种、CD19 + B细胞计数、CD4 + T细胞计数和年龄(适用于该模型)进行调整的模型中,疫苗接种起始时间与接种第二剂疫苗后、接种第三剂疫苗后或研究结束时的高水平抗S IgG滴度无关。值得注意的是,既往移植物抗宿主病(GVHD)或使用免疫抑制药物与高水平抗S IgG滴度无关。≥3级疫苗相关不良事件很少见。
这些数据支持在HCT后三个月开始接种mRNA SARS-CoV-2疫苗,无论是否并发GVHD或使用免疫抑制药物。这是对异基因HCT后第一年针对任何病原体进行疫苗接种的最大规模前瞻性分析之一,并支持目前关于HCT后三个月开始接种SARS-CoV-2疫苗的指南。此外,针对HCT受者中其他病原体的mRNA疫苗制剂的研究很少,这些数据为使用mRNA疫苗平台早期接种针对其他病原体的疫苗的效用提供了令人鼓舞的概念验证。
国家骨髓捐赠项目、白血病和淋巴瘤协会、多发性骨髓瘤研究基金会、诺华公司、LabCorp公司、美国移植和细胞治疗学会、Adaptive Biotechnologies公司以及美国国立卫生研究院。