Interdisciplinary Crohn Colitis Centre Minden, North Rhine-Westphalia, Märchenweg 17, 32429, Minden, Germany.
Real World and Advanced Analytics, Ingress-Health HWM GmbH, Wismar, Mecklenburg-Vorpommern, Germany.
Int J Colorectal Dis. 2023 May 8;38(1):116. doi: 10.1007/s00384-023-04397-7.
Many patients treated for ulcerative colitis (UC) do not achieve clinical remission. This real-world study assessed clinical remission and inadequate response rates among patients with UC in Germany treated with advanced therapies.
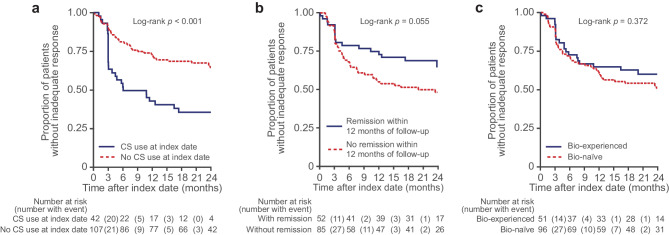
This retrospective chart review included patients with UC newly initiating advanced (index) therapy (anti-TNFα agents, vedolizumab, tofacitinib) from January 2017-September 2019 (index date). Included patients had data for ≥ 12 months before (baseline period) and after the index date (follow-up period). Remission was defined as a partial Mayo score ≤ 1. Indicators of inadequate response were: index therapy discontinuation; therapy adjustments (index therapy dose escalation; augmentation with non-advanced therapies; corticosteroid [CS] use during maintenance therapy); CS dependency (use for ≥ 12 weeks); and UC-related hospitalisation, surgery or emergency department visit. Time to first remission and inadequate response were analyzed using Kaplan-Meier analyses.
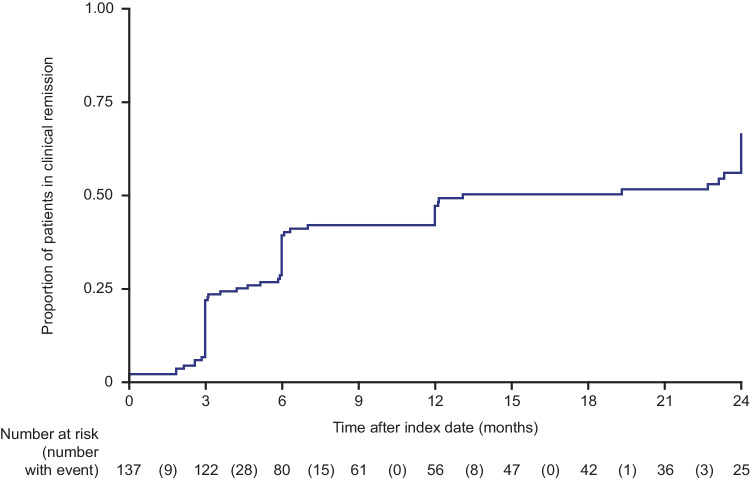
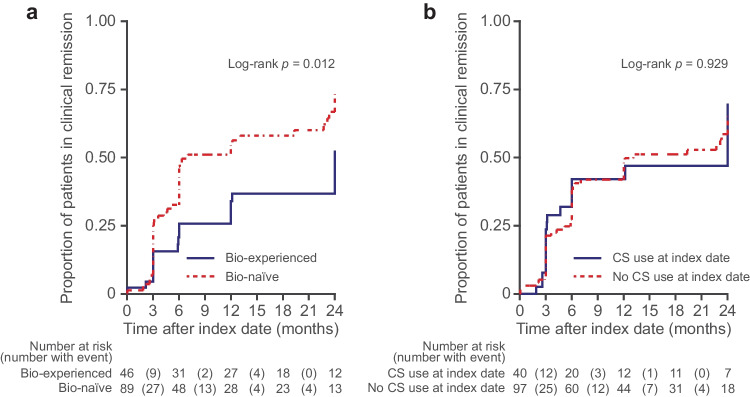
Among 149 patients with UC (median age: 40 years), 96 (64.4%) were biologic-naïve and 42 (28.2%) received CS at the index date. Within 12 months, 52 patients (47.2%) were in remission; of these, 13 patients (25.0%) received ≥ 1 therapy adjustment. At 12 months, 55 patients (37.6%) had ≥ 1 indicator of an inadequate response. Median time to remission was longer among biologic-experienced vs biologic-naïve patients (24 vs 7 months; p = 0.012).
Over half of the patients were not in clinical remission after 12 months and more than one-third experienced inadequate response. One-quarter of patients in remission required therapy adjustments. Patients with UC require therapies that are more effective than those currently available to achieve better treatment outcomes.
许多溃疡性结肠炎(UC)患者未达到临床缓解。本真实世界研究评估了德国接受高级治疗的 UC 患者达到临床缓解和应答不足的比例。
本回顾性图表研究纳入了 2017 年 1 月至 2019 年 9 月期间新开始接受高级(起始)治疗(抗 TNFα 制剂、vedolizumab、tofacitinib)的 UC 患者(起始日期)。纳入的患者在起始日期之前(基线期)和之后(随访期)至少有 12 个月的数据。缓解定义为部分 Mayo 评分≤1。应答不足的指标包括:起始治疗停药;治疗调整(起始治疗剂量升级;非高级治疗的附加治疗;维持治疗时使用皮质类固醇[CS]);CS 依赖性(使用≥12 周);以及与 UC 相关的住院、手术或急诊就诊。采用 Kaplan-Meier 分析评估首次缓解和应答不足的时间。
在 149 例 UC 患者中(中位年龄:40 岁),96 例(64.4%)为生物初治患者,42 例(28.2%)在起始日期时使用 CS。在 12 个月内,52 例(47.2%)患者缓解;其中,13 例(25.0%)患者接受了≥1 次治疗调整。在 12 个月时,55 例(37.6%)患者有≥1 项应答不足的指标。生物治疗经验患者的缓解中位时间长于生物初治患者(24 个月 vs 7 个月;p=0.012)。
超过一半的患者在 12 个月后未达到临床缓解,超过三分之一的患者应答不足。四分之一缓解的患者需要治疗调整。UC 患者需要更有效的治疗方案来实现更好的治疗结局。