Siemensma Mark F, van der Windt Anna E, van Es Eline M, Colaris Joost W, Eygendaal Denise
Erasmus MC, University Medical Center Rotterdam, Department of Orthopaedics and Sports Medicine, 3000 CA, Rotterdam, The Netherlands.
EFORT Open Rev. 2023 May 9;8(5):351-360. doi: 10.1530/EOR-23-0039.
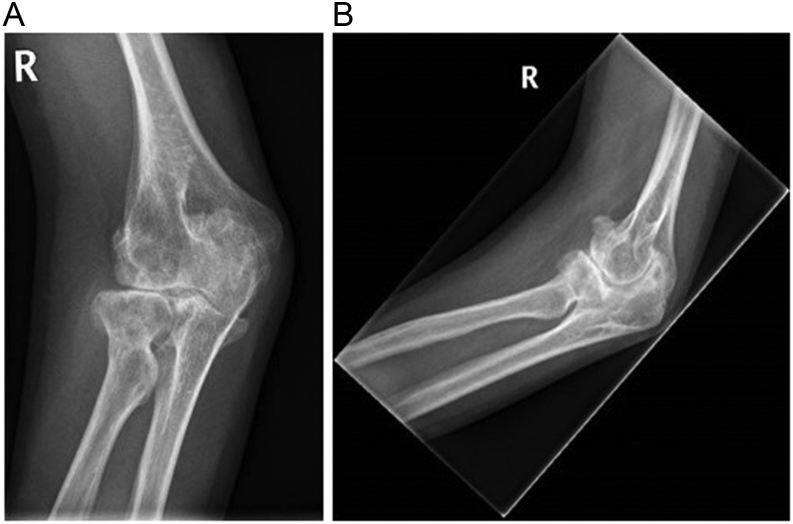
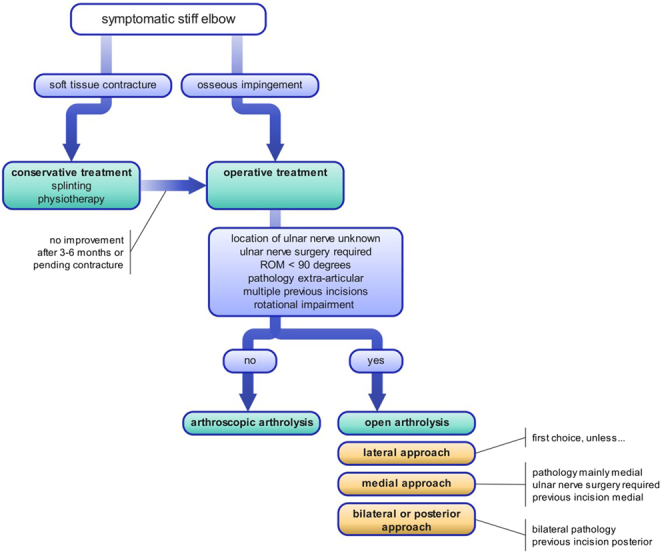
The elbow is prone to stiffness due to its unique anatomy and profound capsular reaction to inflammation. The resulting movement impairment may significantly interfere with a patient's activities of daily living. Trauma (including surgery for trauma), posttraumatic arthritis, and heterotopic ossification (HO) are the most common causes of elbow stiffness. In stiffness caused by soft tissue contractures, initial conservative treatment with physiotherapy (PT) and splinting is advised. In cases in which osseous deformities limit range of motion (e.g. malunion, osseous impingement, or HO), early surgical intervention is recommended. Open and arthroscopic arthrolysis are the primary surgical options. Arthroscopic arthrolysis has a lower complication and revision rate but has narrower indications. Early active mobilization using PT after surgery is recommended in postoperative rehabilitation and may be complemented by splinting or continuous passive motion therapy. Most results are gained within the first few months but can continue to improve until 12 months. This paper reviews the current literature and provides state-of-the-art guidance on the management regarding prevention, evaluation, and treatment of elbow stiffness.
由于肘部独特的解剖结构以及对炎症的强烈关节囊反应,肘部容易出现僵硬。由此导致的活动障碍可能会严重干扰患者的日常生活。创伤(包括创伤手术)、创伤后关节炎和异位骨化(HO)是肘部僵硬最常见的原因。对于软组织挛缩引起的僵硬,建议首先采用物理治疗(PT)和夹板进行保守治疗。在骨畸形限制活动范围的情况下(如骨不连、骨撞击或HO),建议早期进行手术干预。开放和关节镜下关节松解术是主要的手术选择。关节镜下关节松解术的并发症和翻修率较低,但适应症较窄。术后康复建议术后早期使用PT进行积极活动,也可辅以夹板或持续被动运动治疗。大多数效果在最初几个月内获得,但可持续改善至12个月。本文回顾了当前文献,并提供了关于肘部僵硬预防、评估和治疗管理的最新指导。