Center for Cognitive Medicine, Department of Psychiatry and Behavioral Science, Vanderbilt University Medical Center, Nashville, TN, USA.
Department of Psychiatry, University of Pittsburgh, Pittsburgh, PA, USA.
Transl Psychiatry. 2023 May 10;13(1):160. doi: 10.1038/s41398-023-02464-9.
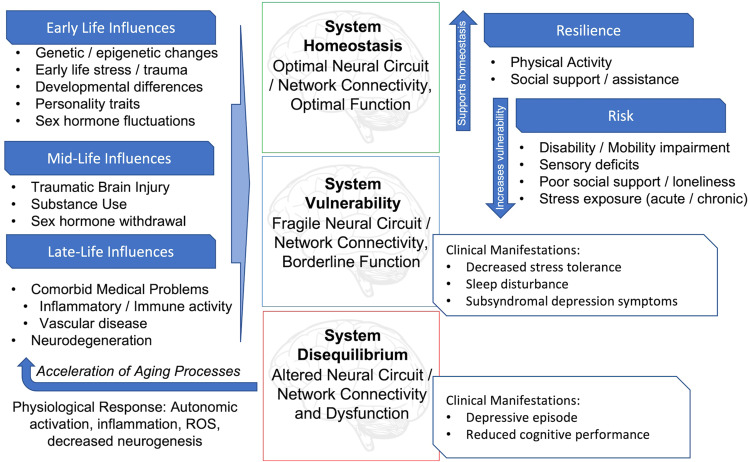
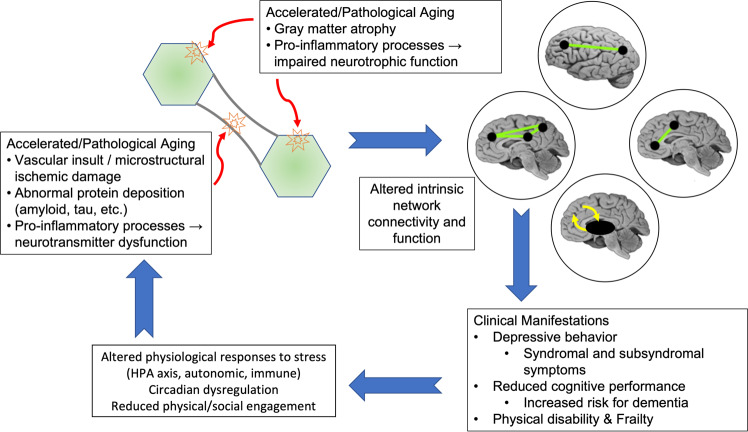
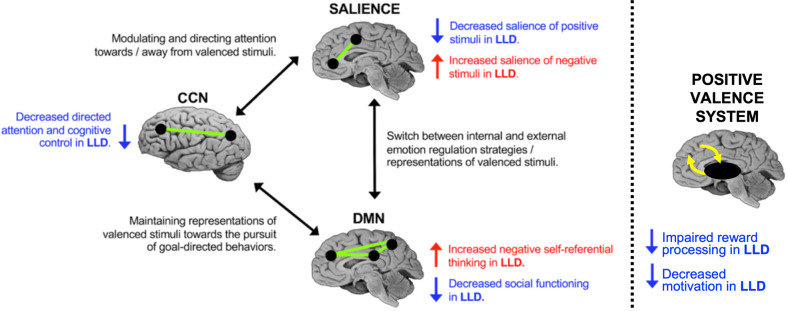
Late-life depression occurring in older adults is common, recurrent, and malignant. It is characterized by affective symptoms, but also cognitive decline, medical comorbidity, and physical disability. This behavioral and cognitive presentation results from altered function of discrete functional brain networks and circuits. A wide range of factors across the lifespan contributes to fragility and vulnerability of those networks to dysfunction. In many cases, these factors occur earlier in life and contribute to adolescent or earlier adulthood depressive episodes, where the onset was related to adverse childhood events, maladaptive personality traits, reproductive events, or other factors. Other individuals exhibit a later-life onset characterized by medical comorbidity, pro-inflammatory processes, cerebrovascular disease, or developing neurodegenerative processes. These later-life processes may not only lead to vulnerability to the affective symptoms, but also contribute to the comorbid cognitive and physical symptoms. Importantly, repeated depressive episodes themselves may accelerate the aging process by shifting allostatic processes to dysfunctional states and increasing allostatic load through the hypothalamic-pituitary-adrenal axis and inflammatory processes. Over time, this may accelerate the path of biological aging, leading to greater brain atrophy, cognitive decline, and the development of physical decline and frailty. It is unclear whether successful treatment of depression and avoidance of recurrent episodes would shift biological aging processes back towards a more normative trajectory. However, current antidepressant treatments exhibit good efficacy for older adults, including pharmacotherapy, neuromodulation, and psychotherapy, with recent work in these areas providing new guidance on optimal treatment approaches. Moreover, there is a host of nonpharmacological treatment approaches being examined that take advantage of resiliency factors and decrease vulnerability to depression. Thus, while late-life depression is a recurrent yet highly heterogeneous disorder, better phenotypic characterization provides opportunities to better utilize a range of nonspecific and targeted interventions that can promote recovery, resilience, and maintenance of remission.
老年人中出现的迟发性抑郁症很常见、反复发作且具有恶性特征。其特征为情感症状,但也有认知能力下降、合并躯体疾病和身体残疾。这种行为和认知表现源自离散功能脑网络和回路功能的改变。在整个生命周期中,广泛的因素会导致这些网络对功能障碍的脆弱性和易损性增加。在许多情况下,这些因素在生命早期就已经存在,并导致青少年或成年早期的抑郁发作,这些发作与不良的童年事件、适应不良的人格特质、生殖事件或其他因素有关。其他患者表现为迟发性发病,特征为合并躯体疾病、促炎过程、脑血管疾病或发展中的神经退行性过程。这些迟发性过程不仅可能导致易感性增加,出现情感症状,还可能导致合并认知和躯体症状。重要的是,反复的抑郁发作本身可能会通过将适应过程转移到功能障碍状态并通过下丘脑-垂体-肾上腺轴和炎症过程增加适应负荷,从而加速衰老过程。随着时间的推移,这可能会加速生物衰老的进程,导致大脑萎缩、认知能力下降以及躯体功能下降和虚弱的发展。目前尚不清楚成功治疗抑郁症和避免反复发作是否会使生物衰老过程重新回到更正常的轨迹。然而,目前的抗抑郁治疗对老年人具有很好的疗效,包括药物治疗、神经调节和心理治疗,这些领域的最新研究为最佳治疗方法提供了新的指导。此外,正在研究许多非药物治疗方法,这些方法利用了弹性因素并降低了患抑郁症的易感性。因此,虽然迟发性抑郁症是一种反复发作但具有高度异质性的疾病,但更好的表型特征分析为更好地利用一系列非特异性和针对性干预措施提供了机会,这些干预措施可以促进康复、恢复和缓解的维持。