Department of Anesthesia, Critical Care and Pain Medicine, Massachusetts General Hospital, Boston, Massachusetts, United States.
Department of Anesthesia, Critical Care and Pain Medicine, Harvard Medical School, Boston, Massachusetts, United States.
J Appl Physiol (1985). 2023 Jun 1;134(6):1496-1507. doi: 10.1152/japplphysiol.00159.2023. Epub 2023 May 11.
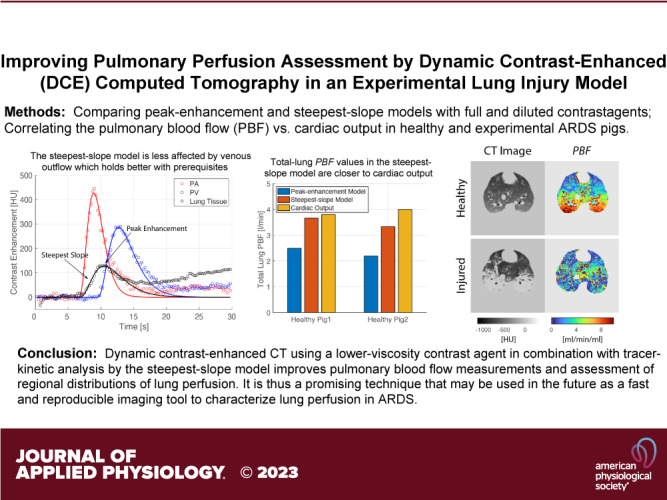
Pulmonary perfusion has been poorly characterized in acute respiratory distress syndrome (ARDS). Optimizing protocols to measure pulmonary blood flow (PBF) via dynamic contrast-enhanced (DCE) computed tomography (CT) could improve understanding of how ARDS alters pulmonary perfusion. In this study, comparative evaluations of injection protocols and tracer-kinetic analysis models were performed based on DCE-CT data measured in ventilated pigs with and without lung injury. Ten Yorkshire pigs (five with lung injury, five healthy) were anesthetized, intubated, and mechanically ventilated; lung injury was induced by bronchial hydrochloric acid instillation. Each DCE-CT scan was obtained during a 30-s end-expiratory breath-hold. Reproducibility of PBF measurements was evaluated in three pigs. In eight pigs, undiluted and diluted Isovue-370 were separately injected to evaluate the effect of contrast viscosity on estimated PBF values. PBF was estimated with the peak-enhancement and the steepest-slope approach. Total-lung PBF was estimated in two healthy pigs to compare with cardiac output measured invasively by thermodilution in the pulmonary artery. Repeated measurements in the same animals yielded a good reproducibility of computed PBF maps. Injecting diluted isovue-370 resulted in smaller contrast-time curves in the pulmonary artery ( < 0.01) and vein ( < 0.01) without substantially diminishing peak signal intensity ( = 0.46 in the pulmonary artery) compared with the pure contrast agent since its viscosity is closer to that of blood. As compared with the peak-enhancement model, PBF values estimated by the steepest-slope model with diluted contrast were much closer to the cardiac output ( = 0.82) as compared with the peak-enhancement model. DCE-CT using the steepest-slope model and diluted contrast agent provided reliable quantitative estimates of PBF. Dynamic contrast-enhanced CT using a lower-viscosity contrast agent in combination with tracer-kinetic analysis by the steepest-slope model improves pulmonary blood flow measurements and assessment of regional distributions of lung perfusion.
在急性呼吸窘迫综合征(ARDS)中,肺部灌注的特征描述较差。通过动态对比增强(DCE)计算机断层扫描(CT)优化测量肺血流量(PBF)的方案,可以更好地了解 ARDS 如何改变肺灌注。在这项研究中,对有和没有肺损伤的通气猪的 DCE-CT 数据进行了注射方案和示踪动力学分析模型的比较评估。十头约克夏猪(五头肺损伤,五头健康)麻醉、插管并机械通气;通过支气管盐酸灌注诱导肺损伤。每个 DCE-CT 扫描都是在 30 秒呼气末屏气期间获得的。在三头猪中评估了 PBF 测量的可重复性。在八头猪中,分别注射未稀释和稀释的 Isovue-370,以评估对比粘度对估计的 PBF 值的影响。使用峰值增强和最陡斜率法估计 PBF。在两只健康猪中估计全肺 PBF,并与肺动脉热稀释法测量的心脏输出进行比较。同一动物的重复测量产生了良好的计算 PBF 图谱的可重复性。与纯造影剂相比,注射稀释的 Isovue-370 可使肺动脉(<0.01)和静脉(<0.01)中的对比时间曲线变小,而峰值信号强度没有明显降低(肺动脉为 0.46),因为其粘度更接近血液。与峰值增强模型相比,用稀释的对比剂通过最陡斜率模型估计的 PBF 值与心脏输出更接近(=0.82),而与峰值增强模型相比。使用最陡斜率模型和低粘度造影剂的 DCE-CT 可提供可靠的 PBF 定量估计。使用低粘度造影剂的动态对比增强 CT 结合最陡斜率模型的示踪动力学分析可改善肺血流量测量和肺灌注的区域性分布评估。