Patterson Jackie K, Ishoso Daniel, Eilevstjønn Joar, Bauserman Melissa, Haug Ingunn, Iyer Pooja, Kamath-Rayne Beena D, Lokangaka Adrien, Lowman Casey, Mafuta Eric, Myklebust Helge, Nolen Tracy, Patterson Janna, Tshefu Antoinette, Bose Carl, Berkelhamer Sara
Department of Pediatrics, University of North Carolina at Chapel Hill, 101 Manning Drive, CB 7596, Chapel Hill, NC 27514, USA.
School of Public Health, University of Kinshasa, Kinshasa 11850, Democratic Republic of the Congo.
Children (Basel). 2023 Mar 30;10(4):652. doi: 10.3390/children10040652.
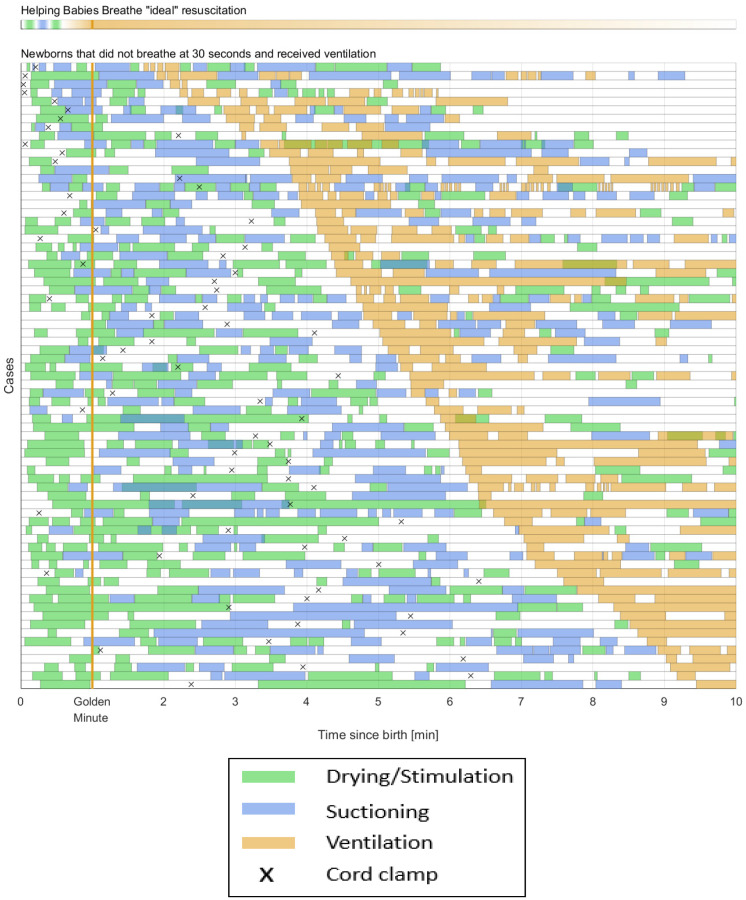
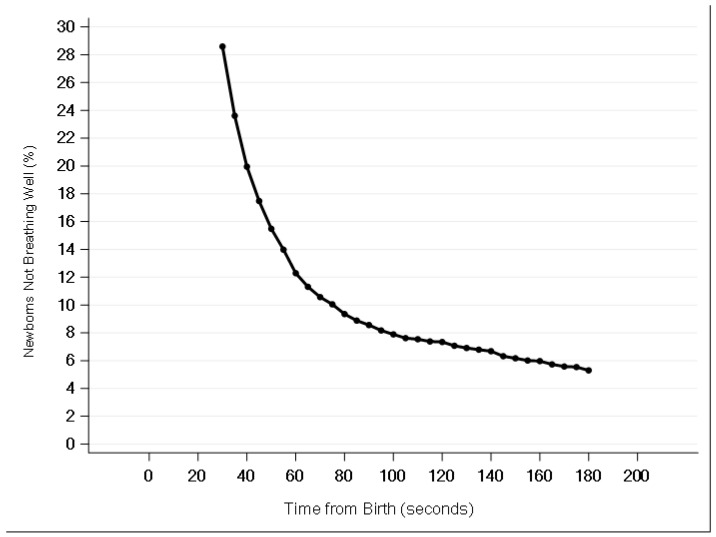
There is a substantial gap in our understanding of resuscitation practices following Helping Babies Breathe (HBB) training. We sought to address this gap through an analysis of observed resuscitations following HBB 2nd edition training in the Democratic Republic of the Congo. This is a secondary analysis of a clinical trial evaluating the effect of resuscitation training and electronic heart rate monitoring on stillbirths. We included in-born, liveborn neonates ≥28 weeks gestation whose resuscitation care was directly observed and documented. For the 2592 births observed, providers dried/stimulated before suctioning in 97% of cases and suctioned before ventilating in 100%. Only 19.7% of newborns not breathing well by 60 s (s) after birth ever received ventilation. Providers initiated ventilation at a median 347 s (>five minutes) after birth; no cases were initiated within the Golden Minute. During 81 resuscitations involving ventilation, stimulation and suction both delayed and interrupted ventilation with a median 132 s spent drying/stimulating and 98 s suctioning. This study demonstrates that HBB-trained providers followed the correct order of resuscitation steps. Providers frequently failed to initiate ventilation. When ventilation was initiated, it was delayed and interrupted by stimulation and suctioning. Innovative strategies targeting early and continuous ventilation are needed to maximize the impact of HBB.
我们对接受“帮助婴儿呼吸”(HBB)培训后的复苏实践的理解存在很大差距。我们试图通过分析在刚果民主共和国进行的HBB第二版培训后观察到的复苏情况来填补这一差距。这是一项对评估复苏培训和电子心率监测对死产影响的临床试验的二次分析。我们纳入了妊娠≥28周的活产新生儿,其复苏护理过程被直接观察和记录。在观察的2592例分娩中,97%的病例中医护人员在吸引前进行了擦干/刺激,100%的病例在通气前进行了吸引。出生后60秒时呼吸不佳的新生儿中,只有19.7%接受了通气。医护人员在出生后中位数347秒(超过5分钟)开始通气;没有病例在黄金一分钟内开始通气。在81次涉及通气的复苏过程中,刺激和吸引都延迟并中断了通气,擦干/刺激的中位数时间为132秒,吸引的中位数时间为98秒。这项研究表明,接受HBB培训的医护人员遵循了正确的复苏步骤顺序。医护人员经常未能开始通气。当开始通气时,通气会被刺激和吸引延迟并中断。需要采取针对早期和持续通气的创新策略,以最大限度地发挥HBB的作用。