Department of International Health, Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland.
Office of HIV/AIDS, United States Agency for International Development, Washington, District of Columbia.
Pediatrics. 2023 Jun 1;151(6). doi: 10.1542/peds.2022-059013.
In 2015, CD4-based clinical staging criteria for antiretroviral therapy (ART) initiation were removed, expanding ART eligibility ("Treat All") for children, who shoulder an outsized burden of HIV-related deaths. To quantify the impact of "Treat All" on pediatric HIV outcomes, we examined shifts in pediatric ART coverage and AIDS mortality before and after "Treat All" implementation.
We abstracted country-level ART coverage (proportion of children <15 years on ART) and AIDS mortality (deaths per 100 000 population) estimates over 11 years. For 91 countries, we also abstracted the year "Treat All" was incorporated into national guidelines. We used multivariable 2-way fixed effects negative binomial regression to estimate changes in pediatric ART coverage and AIDS mortality potentially attributable to "Treat All" expansion, reported as adjusted incidence rate ratios (adj.IRR) with 95% confidence intervals (95% CI).
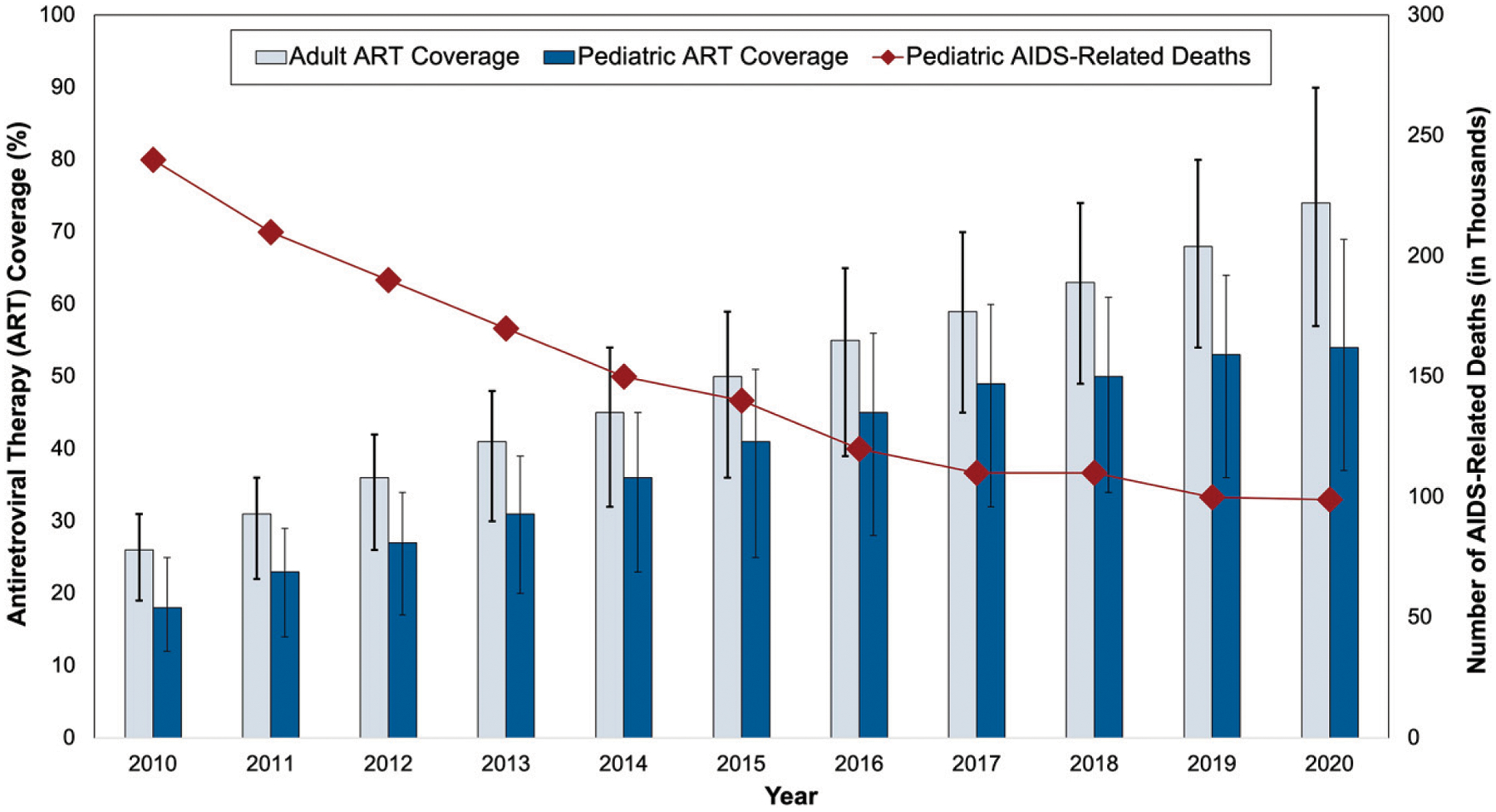
From 2010 to 2020, pediatric ART coverage tripled (16% to 54%), and AIDS-related deaths were halved (240 000 to 99 000). Compared with the pre-implementation period, observed ART coverage continued increasing after "Treat All" adoption, but this rate of increase declined by 6% (adj.IRR = 0.94, 95% CI: 0.91-0.98). AIDS mortality continued declining after "Treat All" adoption, but this rate of decline decreased by 8% (adj.IRR = 1.08, 95% CI: 1.05-1.11) in the post-implementation period.
Although "Treat All" called for increased HIV treatment equity, ART coverage continues lagging in children and comprehensive approaches that address structural issues, including family-based services and intensified case-finding, are needed to close pediatric HIV treatment gaps.
2015 年,取消了基于 CD4 的抗逆转录病毒疗法(ART)启动的临床分期标准,扩大了 ART 的适用范围(“全面治疗”),以覆盖更多的 HIV 相关死亡儿童。为了量化“全面治疗”对儿科 HIV 结局的影响,我们研究了“全面治疗”实施前后儿科 ART 覆盖率和艾滋病死亡率的变化。
我们总结了 11 年来各国的 ART 覆盖率(15 岁以下接受 ART 治疗的儿童比例)和艾滋病死亡率(每 10 万人死亡人数)估计值。对于 91 个国家,我们还总结了“全面治疗”纳入国家指南的年份。我们使用多变量双向固定效应负二项式回归来估计“全面治疗”扩大可能导致的儿科 ART 覆盖率和艾滋病死亡率的变化,以调整后的发病率比(adj.IRR)及其 95%置信区间(95%CI)报告。
从 2010 年到 2020 年,儿科 ART 覆盖率增加了两倍(16%至 54%),艾滋病相关死亡人数减少了一半(24 万至 9.9 万)。与实施前相比,“全面治疗”采用后,观察到的 ART 覆盖率继续增加,但增长率下降了 6%(adj.IRR=0.94,95%CI:0.91-0.98)。“全面治疗”采用后,艾滋病死亡率继续下降,但下降速度在实施后阶段下降了 8%(adj.IRR=1.08,95%CI:1.05-1.11)。
尽管“全面治疗”呼吁增加 HIV 治疗公平性,但儿童的 ART 覆盖率仍然滞后,需要采取综合方法解决结构性问题,包括基于家庭的服务和强化病例发现,以缩小儿科 HIV 治疗差距。