Sax Paul E, Arribas José R, Orkin Chloe, Lazzarin Adriano, Pozniak Anton, DeJesus Edwin, Maggiolo Franco, Stellbrink Hans-Jürgen, Yazdanpanah Yazdan, Acosta Rima, Huang Hailin, Hindman Jason T, Martin Hal, Baeten Jared M, Wohl David
Brigham and Women's Hospital and Harvard Medical School, Boston, MA, USA.
Infectious Diseases Unit, Hospital Universitario La Paz, IdiPaz, CIBERINFEC, Madrid, Spain.
EClinicalMedicine. 2023 May 11;59:101991. doi: 10.1016/j.eclinm.2023.101991. eCollection 2023 May.
Bictegravir/emtricitabine/tenofovir alafenamide (B/F/TAF) is a single-tablet regimen recommended for HIV-1 treatment. The safety and efficacy of B/F/TAF as initial therapy was established in two Phase 3 studies: 1489 (vs dolutegravir [DTG]/abacavir/lamivudine) and 1490 (vs DTG + F/TAF). After 144 weeks of randomized follow-up, an open-label extension evaluated B/F/TAF to 240 weeks.
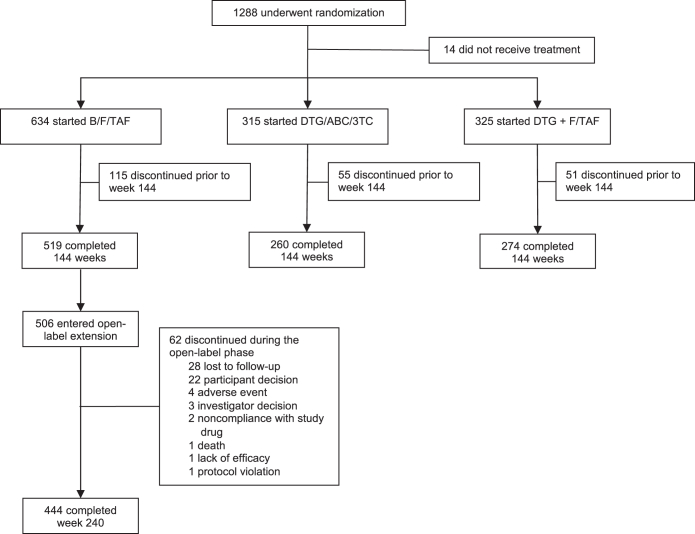
Of 634 participants randomized to B/F/TAF, 519 completed the double-blinded treatment, and 506/634 (80%) chose the 96-week open-label B/F/TAF extension, which was completed by 444/506 (88%) participants. Efficacy was based on the secondary outcome of the proportion of participants with HIV-1 RNA <50 copies/mL at Week 240 by missing = excluded and missing = failure methods. All 634 participants who were randomized to B/F/TAF and received at least one dose of B/F/TAF were included in efficacy and safety analyses. (Study 1489: ClinicalTrials.govNCT02607930; EudraCT 2015-004024-54. Study 1490: ClinicalTrials.govNCT02607956; EudraCT 2015-003988-10).
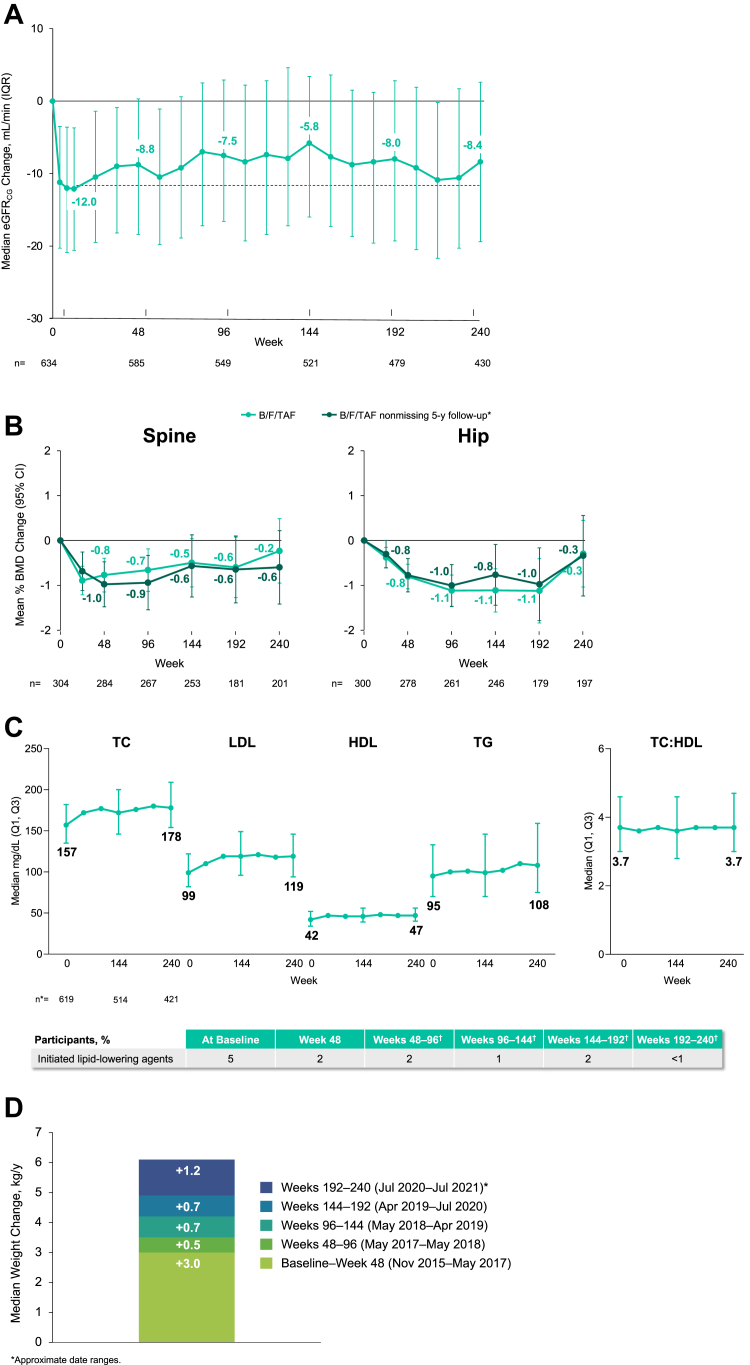
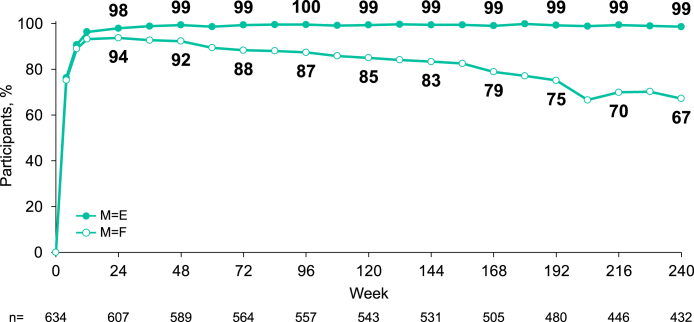
Of those with available virologic data, 98.6% (95% CI [97.0%-99.5%], 426/432) maintained HIV-1 RNA <50 copies/mL at Week 240 (missing = excluded); when missing virologic data were considered as failure, 67.2% (95% CI [63.4%-70.8%], 426/634) maintained HIV-1 RNA <50 copies/mL. Mean (SD) change in CD4+ count from baseline was +338 (236.2) cells/μL. No treatment-emergent resistance to B/F/TAF was detected. Adverse events led to drug discontinuation in 1.6% (n = 10/634) of participants (n = 5 with events considered drug-related). No discontinuations were due to renal adverse events. Median (IQR) total cholesterol increased 21 (1,42) mg/dL from baseline; the change in total cholesterol:HDL was 0.1 (-0.5,0.6) Median (IQR) weight change from baseline was +6.1 kg (2.0, 11.7) at Week 240. In Study 1489, hip and spine bone mineral density mean percent changes from baseline were ≤0.6%.
Through 5 years of follow-up, B/F/TAF maintained high rates of virologic suppression with no treatment-emergent resistance and rare drug discontinuations due to adverse events. These results demonstrate the durability and safety of B/F/TAF in people with HIV.
Gilead Sciences.
比克替拉韦/恩曲他滨/替诺福韦艾拉酚胺(B/F/TAF)是一种推荐用于HIV-1治疗的单片复方制剂。B/F/TAF作为初始治疗的安全性和有效性已在两项3期研究中得到确立:研究1489(与多替拉韦[DTG]/阿巴卡韦/拉米夫定对比)和研究1490(与DTG+F/TAF对比)。在144周的随机随访之后,一项开放标签扩展研究对比克替拉韦/恩曲他滨/替诺福韦艾拉酚胺进行了长达240周的评估。
在634名随机接受B/F/TAF治疗的参与者中,519名完成了双盲治疗,506/634(80%)选择了为期96周的B/F/TAF开放标签扩展治疗,其中444/506(88%)的参与者完成了该治疗。疗效基于240周时HIV-1 RNA<50拷贝/mL的参与者比例这一次要结局,采用缺失值=排除和缺失值=失败两种方法进行计算。所有634名随机接受B/F/TAF治疗且至少接受过一剂B/F/TAF的参与者均纳入疗效和安全性分析。(研究1489:ClinicalTrials.govNCT02607930;EudraCT 2015-004024-54。研究1490:ClinicalTrials.govNCT02607956;EudraCT 2015-003988-10)。
在有可用病毒学数据的参与者中,98.6%(95%CI[97.0%-99.5%],426/432)在240周时维持HIV-1 RNA<50拷贝/mL(缺失值=排除);当将缺失的病毒学数据视为治疗失败时,67.2%(95%CI[63.4%-70.8%],426/634)维持HIV-1 RNA<50拷贝/mL。CD4+细胞计数较基线的平均(标准差)变化为+338(236.2)个/μL。未检测到对B/F/TAF的治疗中出现的耐药。不良事件导致1.6%(n=10/634)的参与者停药(n=5例事件被认为与药物相关)。没有因肾脏不良事件导致的停药。总胆固醇中位数(四分位间距)较基线升高21(1,42)mg/dL;总胆固醇与高密度脂蛋白的变化为0.1(-0.5,0.6)。在240周时,体重较基线的中位数(四分位间距)变化为+6.1 kg(2.0,11.7)。在研究1489中,髋部和脊柱骨密度较基线的平均百分比变化≤0.6%。
经过5年的随访,B/F/TAF维持了较高的病毒学抑制率,未出现治疗中出现的耐药,且因不良事件导致停药的情况罕见。这些结果证明了B/F/TAF在HIV感染者中的持久性和安全性。
吉利德科学公司。