Kaginkar Snehal, Remling-Mulder Leila, Sahoo Ashashree, Pandey Tejaswini, Gurav Pranay, Sutar Jyoti, Singh Amit Kumar, Barnett Ella, Panickan Sivasankar, Akkina Ramesh, Patel Vainav
Viral Immunopathogenesis Laboratory, Indian Council of Medical Research (ICMR)- National Institute for Research in Reproductive and Child Health, Mumbai, India.
Department of Microbiology, Immunology and Pathology, Colorado State University, Fort Collins, CO, United States.
Front Immunol. 2025 Apr 16;16:1552563. doi: 10.3389/fimmu.2025.1552563. eCollection 2025.
While HIV-1 subtype C (HIV-1C) is the most prevalent and widely distributed subtype in the HIV pandemic, nearly all current prevention and therapeutic strategies are based on work with the subtype B (HIV-1B). HIV-1C displays distinct genetic and pathogenic features from that of HIV-1B. Thus, treatment approaches developed for HIV-1B need to be suitably optimized for HIV-1C. A suitable animal model will help delineate comparative aspects of HIV-1C and HIV-1B infections.
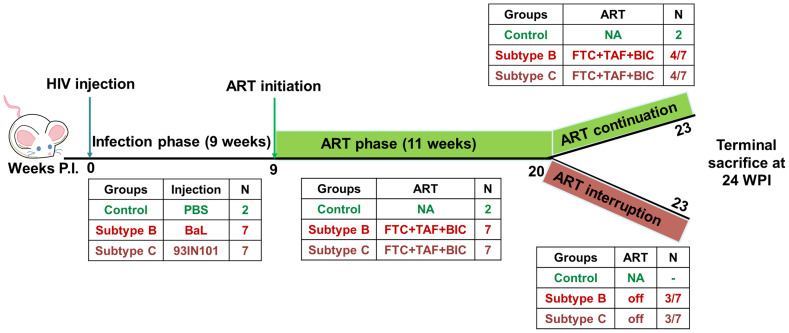
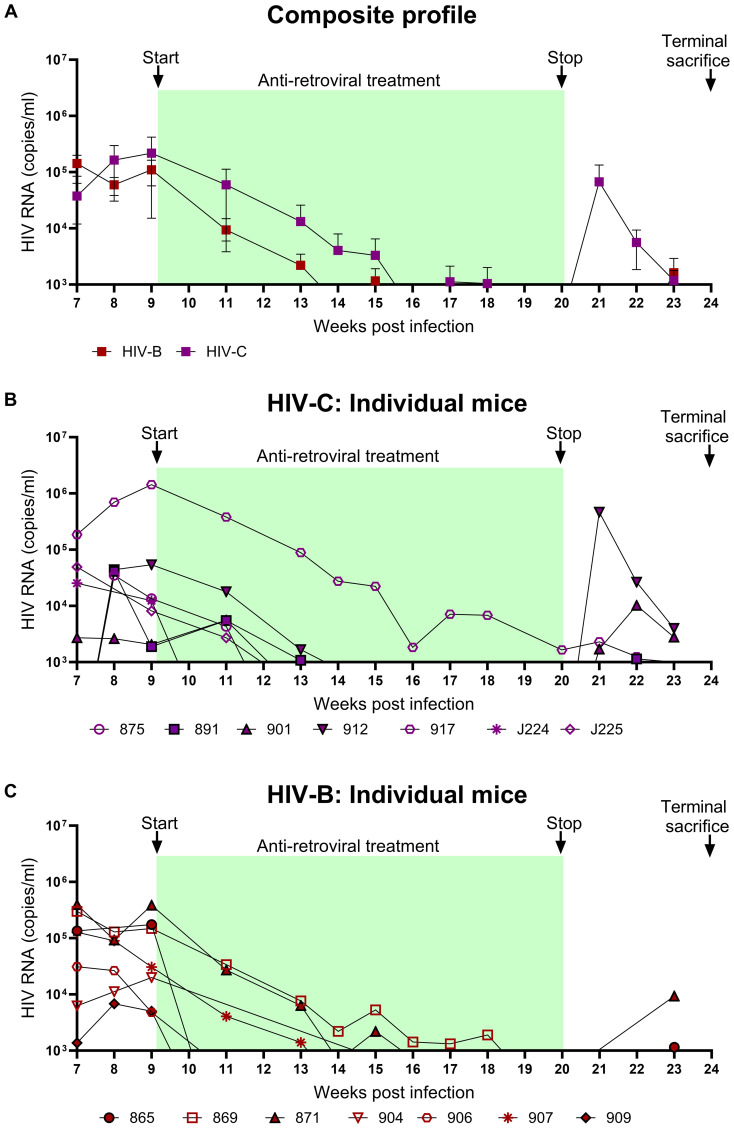
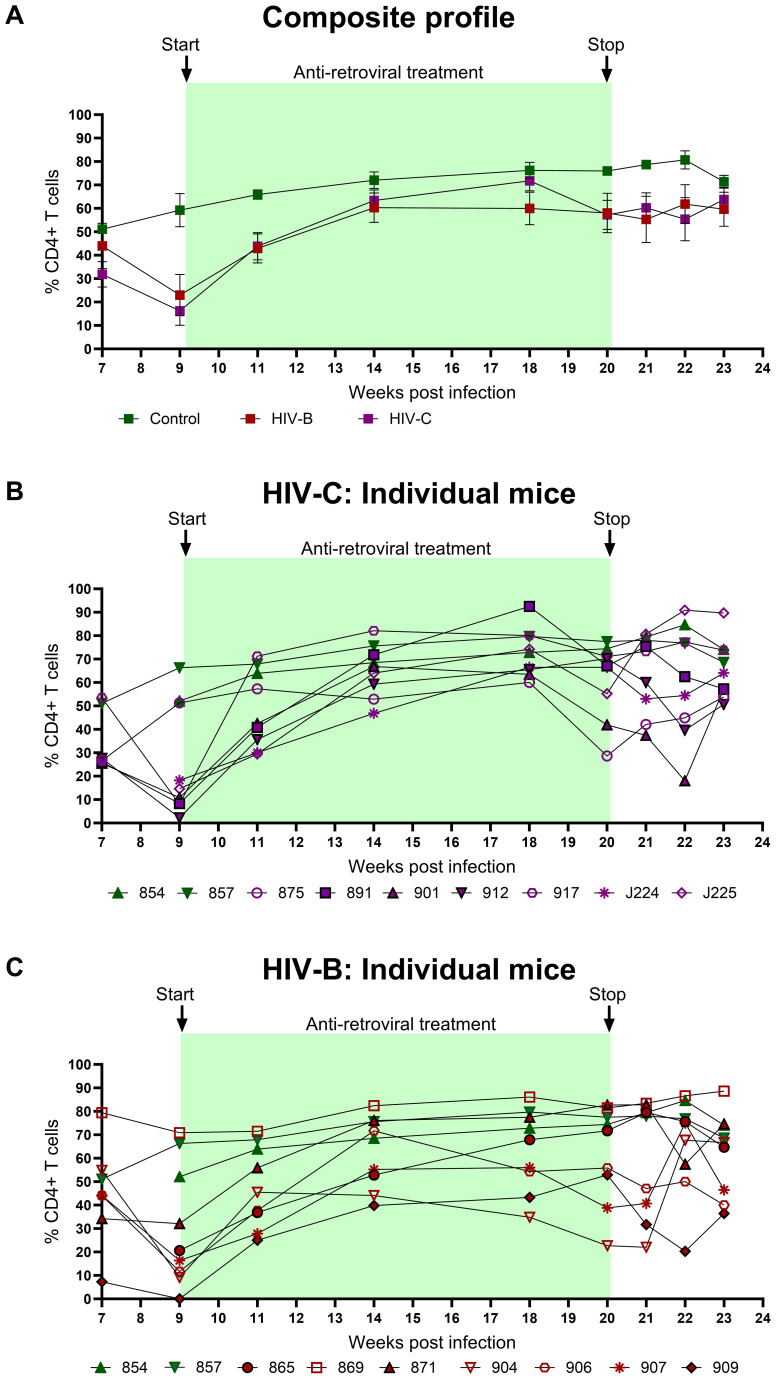
Here, we used a humanized mouse model to evaluate HIV-1C infection, disease progression, response to anti-retroviral therapy (ART) and viral rebound following therapy interruption. A limited comparative study with a prototypical subtype B virus was also performed. Viral infection, immune cell dynamics, acquisition of anti-retroviral therapy (ART) resistance and anatomical reservoir distribution following extended and interrupted therapy were compared.
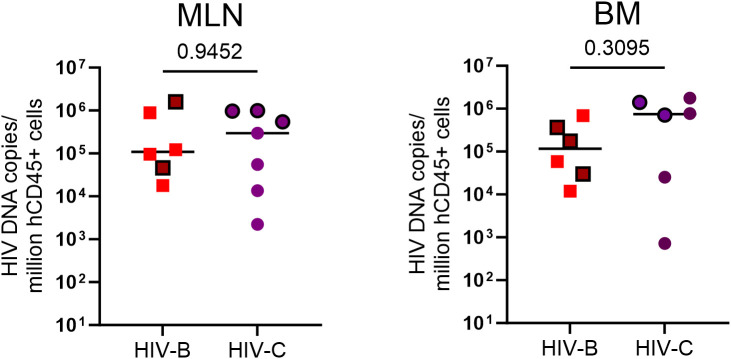
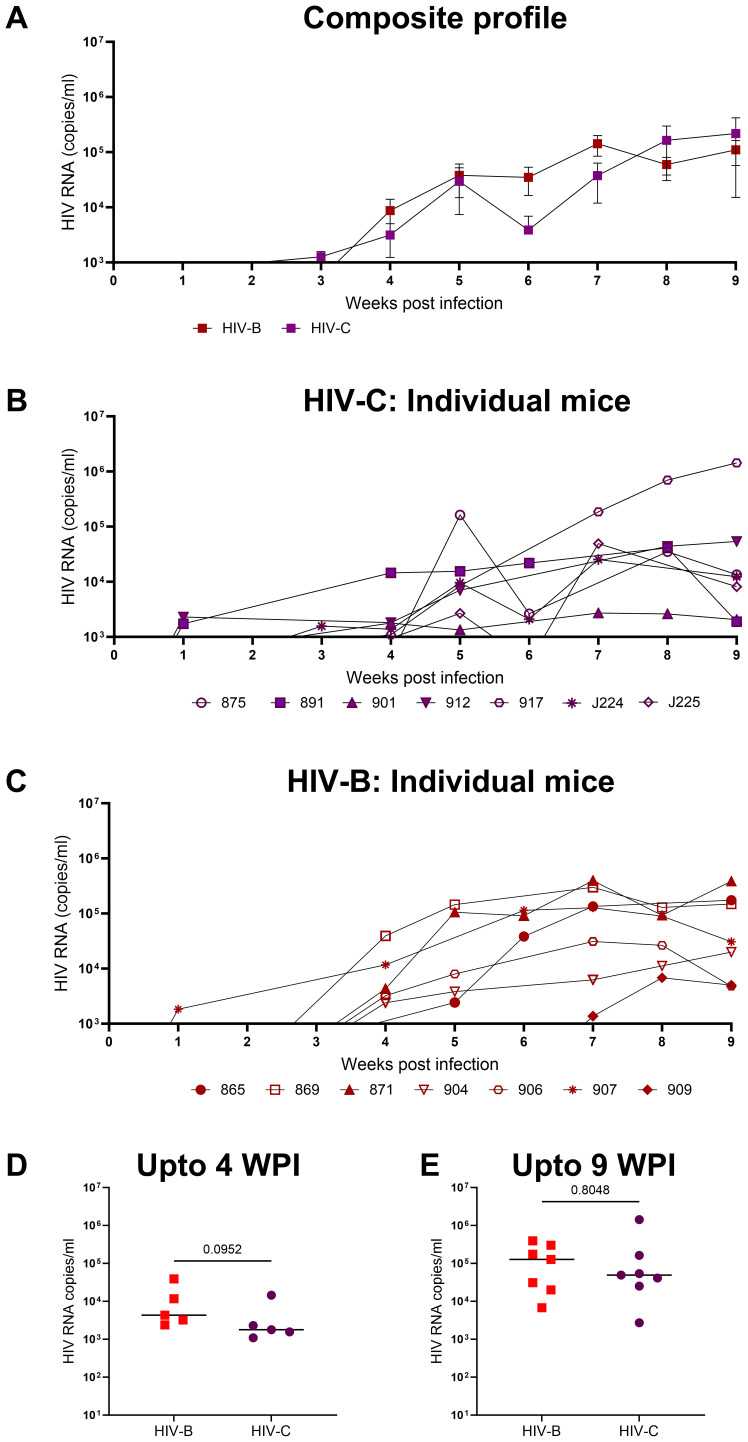
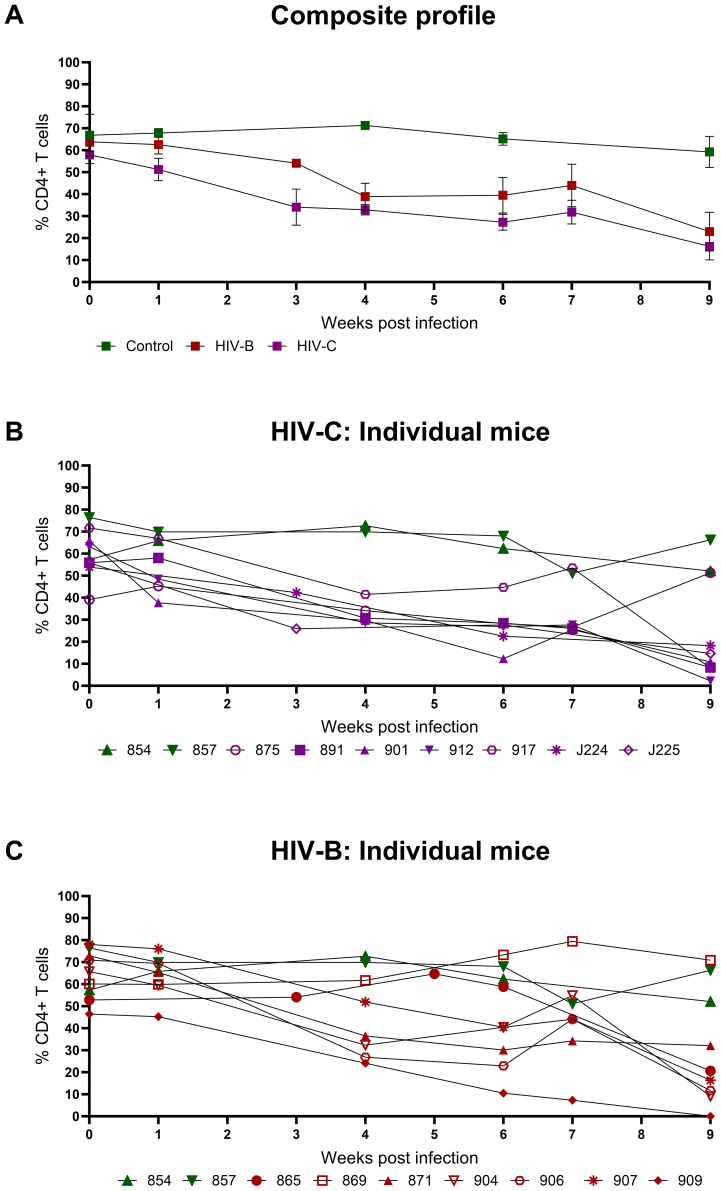
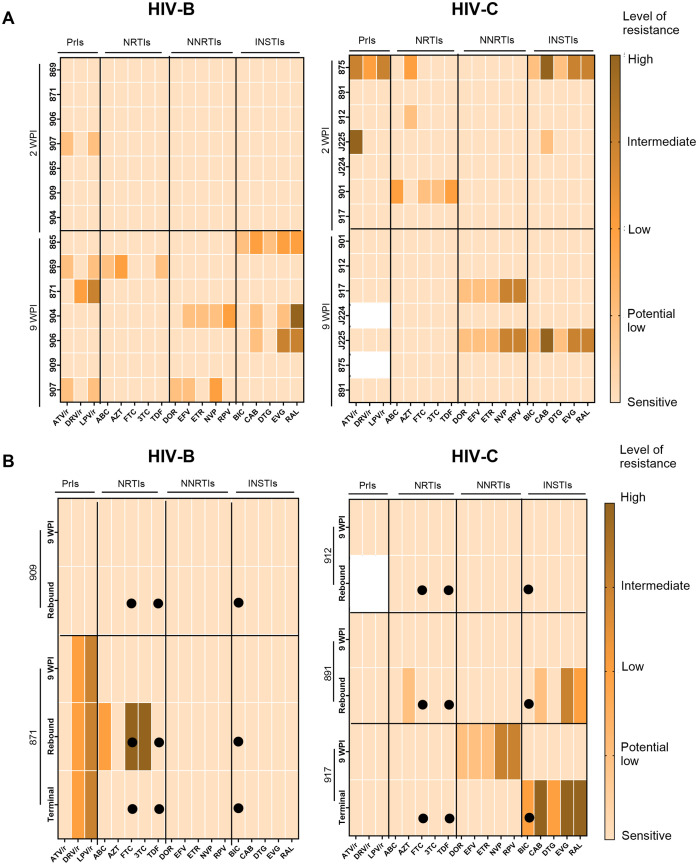
In comparison, lower early plasma viremia was observed with HIV-1C, but with similar rate of CD4+ T cell depletion as that of HIV-1B. Viral suppression by ART was delayed in the HIV-1C infected group with evidence, in one case, of acquired class wide resistance to integrase inhibitors, a critical component of current global therapy regimens. Also, HIV-1C infected animals displayed faster rebound viremia following ART interruption (ATI). Disparate patterns of tissue proviral DNA distribution were observed following extended ART and ATI suggestive of distinct sources of viral rebound.
In this preliminary study, discernible differences were noted between HIV-1C and B with implications for prevention, therapeutics and curative strategies. Results from here also highlight the utility of the hu-HSC mouse model for future expanded studies in this context.
虽然HIV-1 C亚型(HIV-1C)是HIV大流行中最普遍且分布最广泛的亚型,但目前几乎所有的预防和治疗策略都是基于对B亚型(HIV-1B)的研究。HIV-1C与HIV-1B表现出不同的基因和致病特征。因此,为HIV-1B开发的治疗方法需要针对HIV-1C进行适当优化。合适的动物模型将有助于阐明HIV-1C和HIV-1B感染的比较情况。
在此,我们使用人源化小鼠模型来评估HIV-1C感染、疾病进展、对抗逆转录病毒疗法(ART)的反应以及治疗中断后的病毒反弹。还对一种典型的B亚型病毒进行了有限的比较研究。比较了病毒感染、免疫细胞动态、长期和中断治疗后抗逆转录病毒疗法(ART)耐药性的获得情况以及解剖学病毒库分布。
相比之下,HIV-1C感染初期血浆病毒血症较低,但CD4 + T细胞耗竭率与HIV-1B相似。在HIV-1C感染组中,ART对病毒的抑制作用延迟,在一个案例中,有证据表明对整合酶抑制剂产生了全类别的获得性耐药,而整合酶抑制剂是当前全球治疗方案的关键组成部分。此外,HIV-1C感染的动物在ART中断(ATI)后病毒血症反弹更快。在长期ART和ATI后观察到不同的组织前病毒DNA分布模式,提示病毒反弹的来源不同。
在这项初步研究中,注意到HIV-1C和B之间存在明显差异,这对预防、治疗和治愈策略具有影响。此处的结果还突出了人源化造血干细胞(hu-HSC)小鼠模型在这方面未来扩展研究中的实用性。