Department of Rehabilitation Sciences, Faculty of Health, University of Witten/Herdecke, Witten 58455, Germany; DRV Clinic Königsfeld, Center for Medical Rehabilitation, Ennepetal 58256, Germany.
Department of Rehabilitation Sciences, Faculty of Health, University of Witten/Herdecke, Witten 58455, Germany; DRV Clinic Königsfeld, Center for Medical Rehabilitation, Ennepetal 58256, Germany.
Microvasc Res. 2023 Jul;148:104551. doi: 10.1016/j.mvr.2023.104551. Epub 2023 May 16.
Post COVID-19 syndrome (PCS) is a complex condition with partly substantial impact on patients' social and professional life and overall life quality. Currently, the underlying cause(s) of PCS are unknown. Since PCS-specific symptoms could be associated with systemic alterations in tissue oxygen supply, we aimed to investigate changes in tissue oxygenation in patients with PCS.
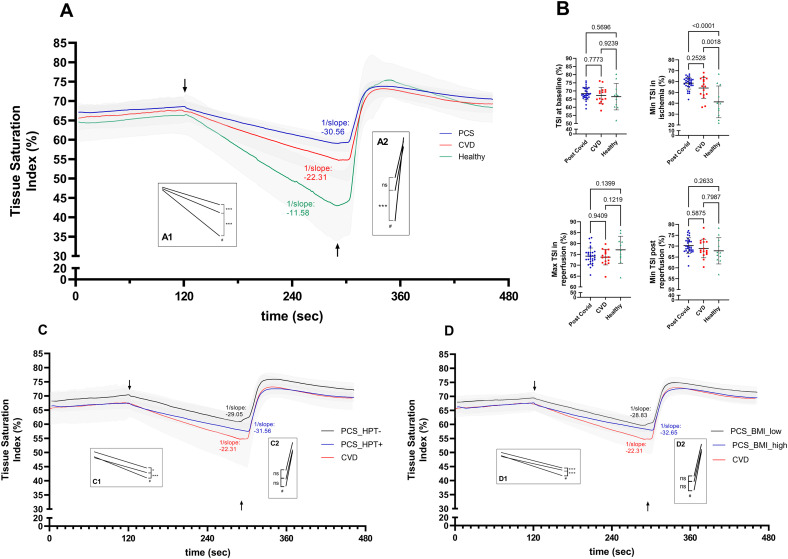
A case-control study including 30 PCS patients (66.6 % males, 48.6 ± 11.2 years, mean time after (first) acute infection: 324 days), 16 cardiologic patients (CVD) (65.5 % males, 56.7 ± 6.3 years) and 11 young healthy controls (55 % males, 28.5 ± 7.4 years) was conducted. Near infrared spectroscopy (NIRS) was used to assess changes in tissue oxygenation during an arterial occlusion protocol on the non-dominant forearm (brachioradialis, 760/850 nm, 5 Hz). The protocol included 10-min rest, a 2-min baseline measurement followed by a 3-min ischemic period (upper-arm cuff, 50 mmHg above resting systolic blood pressure) and a 3-min reoxygenation period. PCS patients were grouped by presence of arterial hypertension and elevated BMI to assess the impact of risk factors.
No differences in mean tissue oxygenation in the pre-occlusion phase existed between groups (p ≥ 0.566). During ischemia, comparisons of linear regressions slopes revealed slower oxygen desaturation for PCS patients (-0.064 %/s) compared to CVD patients (-0.08 %/s) and healthy subjects (-0.145 %/s) (p < 0.001). After cuff release, slowest speed for reoxygenation was detected in PCS patients at 0.84 %/s compared to CVD patients (1.04 %/s) and healthy controls (CG: 2.07 %/s) (p < 0.001). The differences between PCS patients and CVD patients during ischemia remained significant also after correction for risk factors. Analyses of complications during acute infection, persistence of PCS symptoms (time after acute infection), or PCS severity (number of lead symptoms) as confounding factors did not reveal a significant effect.
This study provides evidence that the rate of tissue oxygen consumption is persistently altered in PCS and that PCS patients show an even slower decline in tissue oxygenation during occlusion than CVD patients. Our observations may at least partly explain PCS-specific symptoms such as physical impairment and fatigue.
新冠后综合征(PCS)是一种复杂的病症,部分患者的社会和职业生活以及整体生活质量受到了实质性影响。目前,PCS 的根本原因尚不清楚。由于 PCS 的特定症状可能与组织氧供应的全身改变有关,我们旨在研究 PCS 患者的组织氧合变化。
本病例对照研究纳入了 30 名 PCS 患者(66.6%为男性,48.6±11.2 岁,首次急性感染后平均时间:324 天)、16 名心血管病患者(CVD)(65.5%为男性,56.7±6.3 岁)和 11 名年轻健康对照者(55%为男性,28.5±7.4 岁)。采用近红外光谱(NIRS)技术评估非优势前臂(肱桡肌,760/850nm,5Hz)在动脉闭塞方案期间组织氧合的变化。该方案包括 10 分钟休息、2 分钟基线测量,随后进行 3 分钟缺血期(袖带充气至高于休息时收缩压 50mmHg)和 3 分钟再氧合期。根据是否存在动脉高血压和 BMI 升高将 PCS 患者进行分组,以评估危险因素的影响。
在闭塞前阶段,各组之间的平均组织氧合没有差异(p≥0.566)。在缺血期间,线性回归斜率的比较显示,与 CVD 患者(-0.08%/s)和健康受试者(-0.145%/s)相比,PCS 患者的氧饱和度下降速度较慢(-0.064%/s)(p<0.001)。袖带释放后,PCS 患者的再氧合速度最慢,为 0.84%/s,而 CVD 患者为 1.04%/s,健康对照组为 CG:2.07%/s(p<0.001)。在对危险因素进行校正后,PCS 患者与 CVD 患者在缺血期间的差异仍然显著。对急性感染期间的并发症、PCS 症状的持续存在(急性感染后时间)或 PCS 严重程度(主要症状数量)作为混杂因素进行分析,未发现显著影响。
本研究提供的证据表明,PCS 患者的组织耗氧量持续改变,且与 CVD 患者相比,PCS 患者在闭塞期间的组织氧合下降速度更慢。我们的观察结果至少可以部分解释 PCS 的特定症状,如身体功能障碍和疲劳。