Department of Oncology, University of Gothenburg Institute of Clinical Sciences, Goteborg, Sweden
Department of Radiation Oncology, UCSF, San Francisco, California, USA.
J Immunother Cancer. 2023 May;11(5). doi: 10.1136/jitc-2022-006618.
The implementation of immunological biomarkers for radiotherapy (RT) individualization in breast cancer requires consideration of tumor-intrinsic factors. This study aimed to investigate whether the integration of histological grade, tumor-infiltrating lymphocytes (TILs), programmed cell death protein-1 (PD-1), and programmed death ligand-1 (PD-L1) can identify tumors with aggressive characteristics that can be downgraded regarding the need for RT.
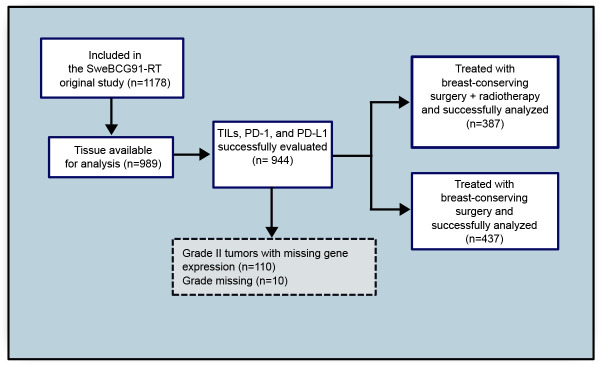
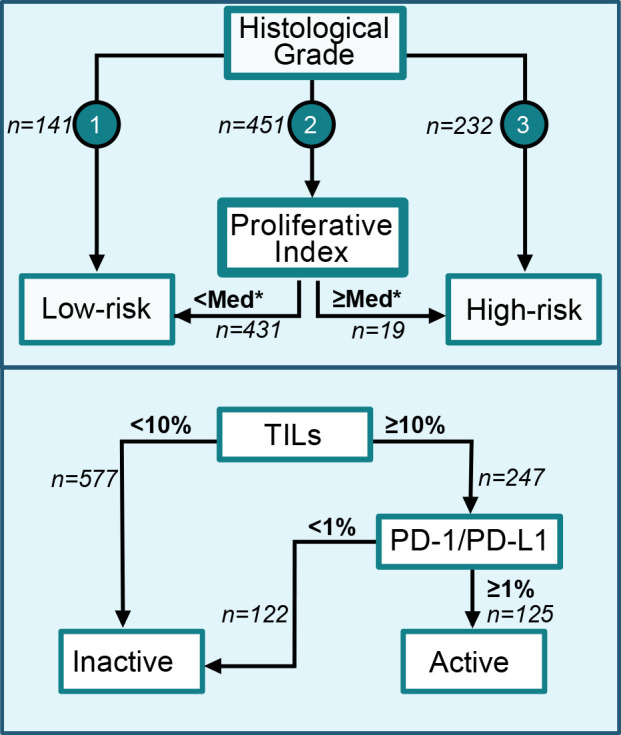
The SweBCG91RT trial included 1178 patients with stage I-IIA breast cancer, randomized to breast-conserving surgery with or without adjuvant RT, and followed for a median time of 15.2 years. Immunohistochemical analyses of TILs, PD-1, and PD-L1 were performed. An activated immune response was defined as stromal TILs ≥10% and PD-1 and/or PD-L1 expression in ≥1% of lymphocytes. Tumors were categorized as high-risk or low-risk using assessments of histological grade and proliferation as measured by gene expression. The risk of ipsilateral breast tumor recurrence (IBTR) and benefit of RT were then analyzed with 10 years follow-up based on the integration of immune activation and tumor-intrinsic risk group.
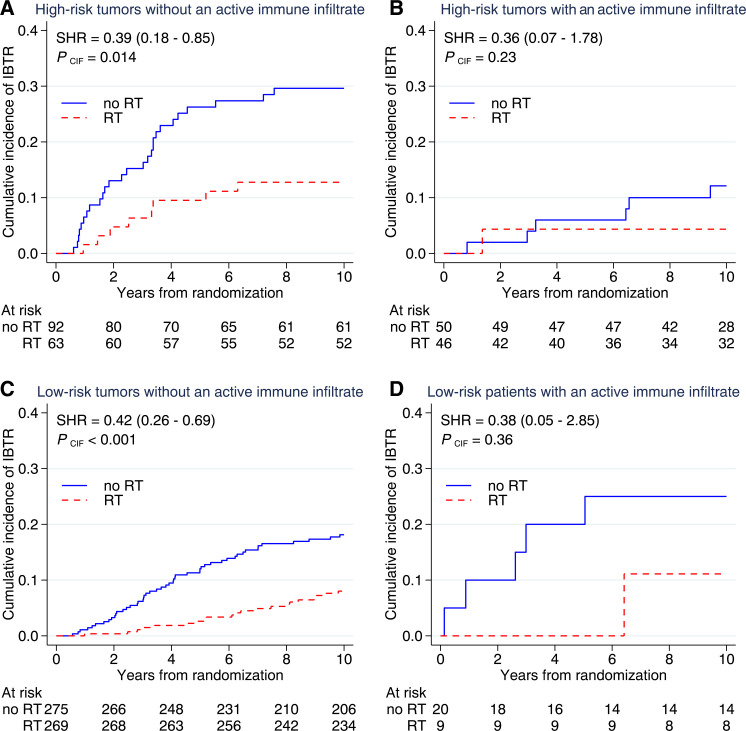
Among high-risk tumors, an activated immune infiltrate was associated with a reduced risk of IBTR (HR 0.34, 95% CI 0.16 to 0.73, p=0.006). The incidence of IBTR in this group was 12.1% (5.6-25.0) without RT and 4.4% (1.1-16.3) with RT. In contrast, the incidence of IBTR in the high-risk group without an activated immune infiltrate was 29.6% (21.4-40.2) without RT and 12.8% (6.6-23.9) with RT. Among low-risk tumors, no evidence of a favorable prognostic effect of an activated immune infiltrate was seen (HR 2.0, 95% CI 0.87 to 4.6, p=0.100).
Integrating histological grade and immunological biomarkers can identify tumors with aggressive characteristics but a low risk of IBTR despite a lack of RT boost and systemic therapy. Among high-risk tumors, the risk reduction of IBTR conferred by an activated immune infiltrate is comparable to treatment with RT. These findings may apply to cohorts dominated by estrogen receptor-positive tumors.
在乳腺癌的放疗个体化中实施免疫生物标志物需要考虑肿瘤内在因素。本研究旨在探讨整合组织学分级、肿瘤浸润淋巴细胞(TILs)、程序性细胞死亡蛋白-1(PD-1)和程序性死亡配体-1(PD-L1)是否可以识别具有侵袭性特征的肿瘤,这些肿瘤可以降级考虑是否需要放疗。
SweBCG91RT 试验纳入了 1178 例 I 期-IIA 期乳腺癌患者,随机分为保乳手术加或不加辅助放疗,并随访中位时间为 15.2 年。对 TILs、PD-1 和 PD-L1 进行了免疫组织化学分析。将间质 TILs≥10%和/或淋巴细胞中 PD-1 和/或 PD-L1 表达≥1%定义为激活的免疫反应。利用基因表达评估的组织学分级和增殖对肿瘤进行高风险或低风险分类。然后,基于免疫激活和肿瘤内在风险组的整合,在 10 年随访时分析同侧乳腺肿瘤复发(IBTR)的风险和放疗的获益。
在高风险肿瘤中,激活的免疫浸润与降低 IBTR 风险相关(HR 0.34,95%CI 0.16 至 0.73,p=0.006)。该组无放疗时的 IBTR 发生率为 12.1%(5.6-25.0),有放疗时为 4.4%(1.1-16.3)。相比之下,在高风险组中,如果没有激活的免疫浸润,IBTR 的发生率为无放疗时的 29.6%(21.4-40.2)和有放疗时的 12.8%(6.6-23.9)。在低风险肿瘤中,没有证据表明激活的免疫浸润具有有利的预后作用(HR 2.0,95%CI 0.87 至 4.6,p=0.100)。
整合组织学分级和免疫生物标志物可以识别具有侵袭性特征但 IBTR 风险较低的肿瘤,尽管没有放疗增强和全身治疗。在高风险肿瘤中,激活的免疫浸润降低 IBTR 的风险可与放疗相媲美。这些发现可能适用于以雌激素受体阳性肿瘤为主的队列。