Department of Surgery, Amsterdam UMC, University of Amsterdam, Amsterdam, The Netherlands.
Cancer Center Amsterdam, Amsterdam, The Netherlands.
Ann Surg Oncol. 2023 Aug;30(8):5051-5060. doi: 10.1245/s10434-023-13465-9. Epub 2023 May 20.
Surgeons aim for R0 resection in patients with pancreatic cancer to improve overall survival. However, it is unclear whether recent changes in pancreatic cancer care such as centralization, increased use of neoadjuvant therapy, minimally invasive surgery, and standardized pathology reporting have influenced R0 resections and whether R0 resection remains associated with overall survival.
This nationwide retrospective cohort study included consecutive patients after pancreatoduodenectomy (PD) for pancreatic cancer from the Netherlands Cancer Registry and the Dutch Nationwide Pathology Database (2009-2019). R0 resection was defined as > 1 mm tumor clearance at the pancreatic, posterior, and vascular resection margins. Completeness of pathology reporting was scored on the basis of six elements: histological diagnosis, tumor origin, radicality, tumor size, extent of invasion, and lymph node examination.
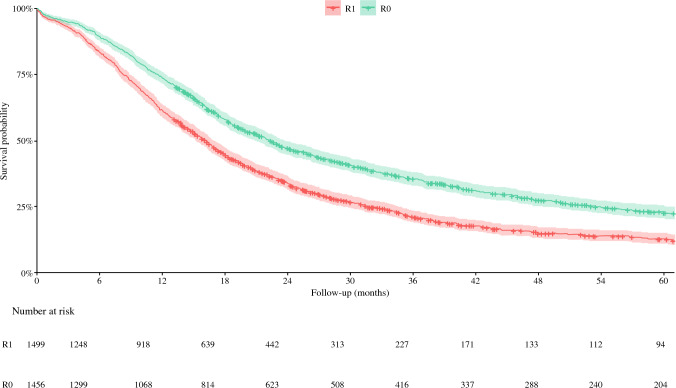
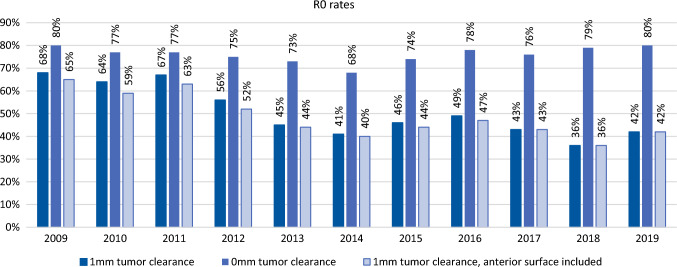
Among 2955 patients after PD for pancreatic cancer, the R0 resection rate was 49%. The R0 resection rate decreased from 68 to 43% (2009-2019, P < 0.001). The extent of resections in high-volume hospitals, minimally invasive surgery, neoadjuvant therapy, and complete pathology reports all significantly increased over time. Only complete pathology reporting was independently associated with lower R0 rates (OR 0.76, 95% CI 0.69-0.83, P < 0.001). Higher hospital volume, neoadjuvant therapy, and minimally invasive surgery were not associated with R0. R0 resection remained independently associated with improved overall survival (HR 0.72, 95% CI 0.66-0.79, P < 0.001), as well as in the 214 patients after neoadjuvant treatment (HR 0.61, 95% CI 0.42-0.87, P = 0.007).
The nationwide rate of R0 resections after PD for pancreatic cancer decreased over time, mostly related to more complete pathology reporting. R0 resection remained associated with overall survival.
外科医生在治疗胰腺癌患者时力求达到 R0 切除,以提高总体生存率。然而,目前尚不清楚胰腺癌治疗方面的最近变化,如集中化、新辅助治疗的增加、微创手术以及标准化病理报告是否会影响 R0 切除,以及 R0 切除是否仍然与总体生存率相关。
本项全国性回顾性队列研究纳入了荷兰癌症登记处和荷兰全国病理数据库中连续接受胰十二指肠切除术(PD)治疗的胰腺癌患者(2009-2019 年)。R0 切除定义为胰腺、后方和血管切缘的肿瘤清除>1mm。病理报告的完整性基于六个要素进行评分:组织学诊断、肿瘤起源、根治性、肿瘤大小、侵犯范围和淋巴结检查。
在 2955 例接受 PD 治疗的胰腺癌患者中,R0 切除率为 49%。R0 切除率从 68%降至 43%(2009-2019 年,P<0.001)。高容量医院的手术范围、微创手术、新辅助治疗和完整的病理报告均随着时间的推移显著增加。只有完整的病理报告与较低的 R0 率独立相关(OR 0.76,95%CI 0.69-0.83,P<0.001)。更高的医院容量、新辅助治疗和微创手术与 R0 无关。R0 切除仍然与总体生存率的提高独立相关(HR 0.72,95%CI 0.66-0.79,P<0.001),在接受新辅助治疗的 214 例患者中也是如此(HR 0.61,95%CI 0.42-0.87,P=0.007)。
全国范围内 PD 治疗胰腺癌的 R0 切除率随时间推移而下降,主要与更完整的病理报告有关。R0 切除仍然与总体生存率相关。