National Amyloidosis Centre, University College London, Royal Free Campus, Rowland Hill Street, London NW3 2PF, UK.
Center for Diagnosis and Treatment of Cardiomyopathies, Cardiovascular Department, Azienda Sanitaria Universitaria Giuliano-Isontina (ASUGI), University of Trieste, Via Giacomo Puccini, Trieste 34100, Italy.
Eur Heart J. 2023 Aug 14;44(31):2893-2907. doi: 10.1093/eurheartj/ehad347.
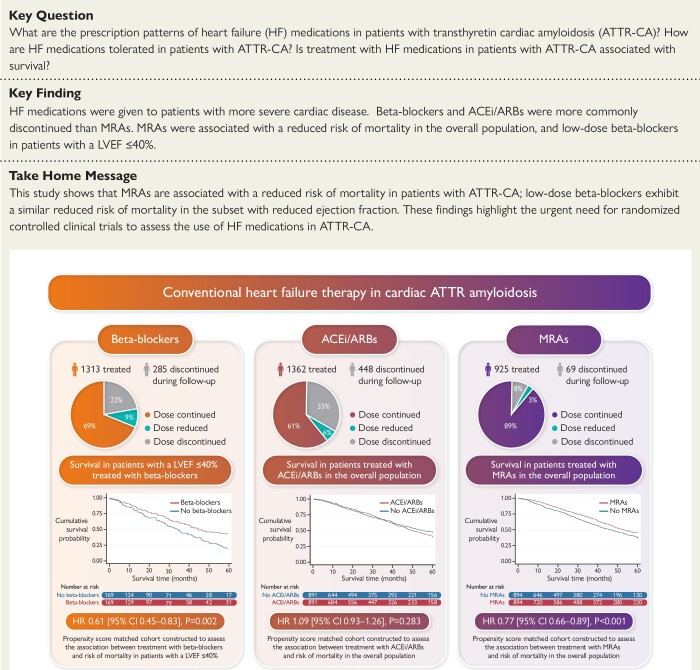
The aims of this study were to assess prescription patterns, dosages, discontinuation rates, and association with prognosis of conventional heart failure medications in patients with transthyretin cardiac amyloidosis (ATTR-CA).
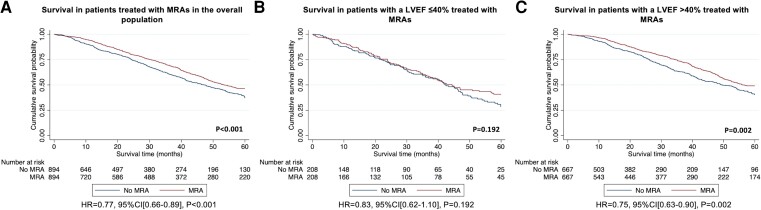
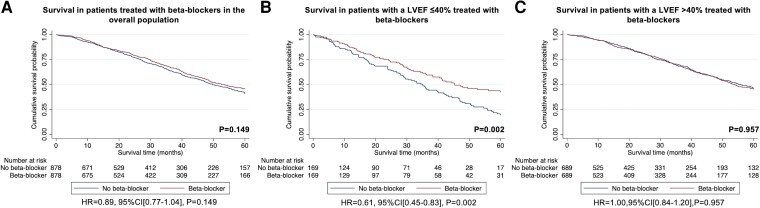
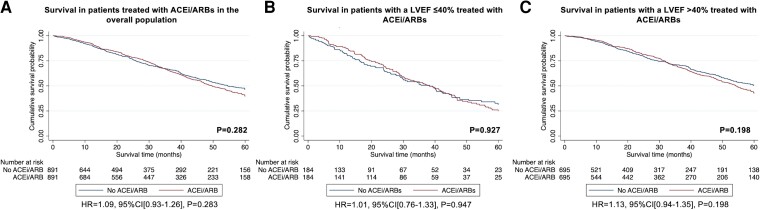
A retrospective analysis of all consecutive patients diagnosed with ATTR-CA at the National Amyloidosis Centre between 2000 and 2022 identified 2371 patients with ATTR-CA. Prescription of heart failure medications was greater among patients with a more severe cardiac phenotype, comprising beta-blockers in 55.4%, angiotensin-converting enzyme inhibitors (ACEis)/angiotensin II receptor blockers (ARBs) in 57.4%, and mineralocorticoid receptor antagonists (MRAs) in 39.0% of cases. During a median follow-up of 27.8 months (interquartile range 10.6-51.3), 21.7% had beta-blockers discontinued, and 32.9% had ACEi/ARBs discontinued. In contrast, only 7.5% had MRAs discontinued. A propensity score-matched analysis demonstrated that treatment with MRAs was independently associated with a reduced risk of mortality in the overall population [hazard ratio (HR) 0.77 (95% confidence interval (CI) 0.66-0.89), P < .001] and in a pre-specified subgroup of patients with a left ventricular ejection fraction (LVEF) >40% [HR 0.75 (95% CI 0.63-0.90), P = .002]; and treatment with low-dose beta-blockers was independently associated with a reduced risk of mortality in a pre-specified subgroup of patients with a LVEF ≤40% [HR 0.61 (95% CI 0.45-0.83), P = .002]. No convincing differences were found for treatment with ACEi/ARBs.
Conventional heart failure medications are currently not widely prescribed in ATTR-CA, and those that received medication had more severe cardiac disease. Beta-blockers and ACEi/ARBs were often discontinued, but low-dose beta-blockers were associated with reduced risk of mortality in patients with a LVEF ≤40%. In contrast, MRAs were rarely discontinued and were associated with reduced risk of mortality in the overall population; but these findings require confirmation in prospective randomized controlled trials.
本研究旨在评估转甲状腺素蛋白心脏淀粉样变(ATTR-CA)患者常规心力衰竭药物的处方模式、剂量、停药率及与预后的关系。
对 2000 年至 2022 年在国家淀粉样变性中心连续诊断为 ATTR-CA 的所有患者进行回顾性分析,共纳入 2371 例 ATTR-CA 患者。具有更严重心脏表型的患者更常开心力衰竭药物,包括 55.4%的β受体阻滞剂、57.4%的血管紧张素转换酶抑制剂(ACEi)/血管紧张素 II 受体阻滞剂(ARB)和 39.0%的盐皮质激素受体拮抗剂(MRA)。中位随访 27.8 个月(四分位间距 10.6-51.3)期间,21.7%的患者停用了β受体阻滞剂,32.9%的患者停用了 ACEi/ARB。相比之下,只有 7.5%的患者停用了 MRA。倾向性评分匹配分析表明,在总体人群中,MRA 治疗与降低死亡率风险独立相关[风险比(HR)0.77(95%置信区间(CI)0.66-0.89),P<0.001],在左心室射血分数(LVEF)>40%的预先指定亚组中也与降低死亡率风险相关[HR 0.75(95%CI 0.63-0.90),P=0.002];而在预先指定的 LVEF≤40%的亚组中,低剂量β受体阻滞剂治疗与降低死亡率风险独立相关[HR 0.61(95%CI 0.45-0.83),P=0.002]。ACEi/ARB 的治疗效果没有明显差异。
目前,常规心力衰竭药物在 ATTR-CA 中并未广泛应用,而接受药物治疗的患者心脏疾病更严重。β受体阻滞剂和 ACEi/ARB 常被停用,但在 LVEF≤40%的患者中,低剂量β受体阻滞剂与降低死亡率风险相关。相反,MRA 很少被停用,与总体人群的死亡率降低相关;但这些发现需要前瞻性随机对照试验来证实。