Brewerton Timothy D
Department of Psychiatry and Behavioral Sciences, Medical University of South Carolina, Charleston, SC, United States.
Front Psychiatry. 2023 May 12;14:1149433. doi: 10.3389/fpsyt.2023.1149433. eCollection 2023.
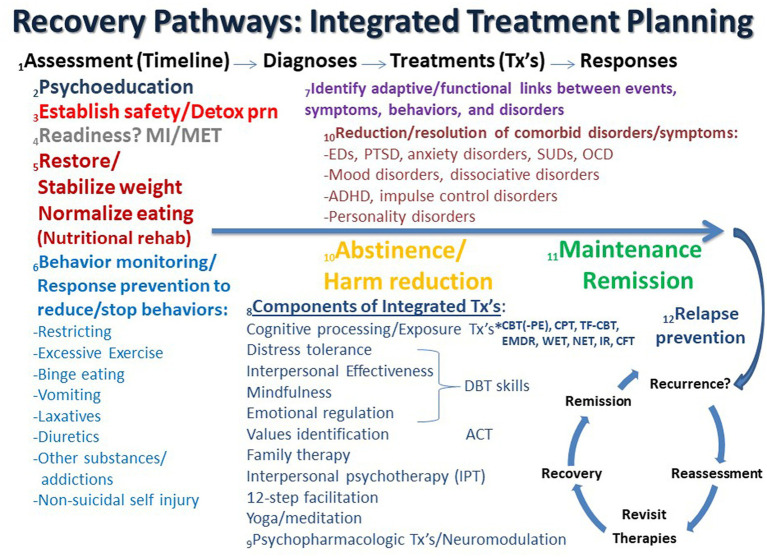
Psychiatric comorbidity is the norm in the assessment and treatment of eating disorders (EDs), and traumatic events and lifetime PTSD are often major drivers of these challenging complexities. Given that trauma, PTSD, and psychiatric comorbidity significantly influence ED outcomes, it is imperative that these problems be appropriately addressed in ED practice guidelines. The presence of associated psychiatric comorbidity is noted in some but not all sets of existing guidelines, but they mostly do little to address the problem other than referring to independent guidelines for other disorders. This disconnect perpetuates a "silo effect," in which each set of guidelines do not address the complexity of the other comorbidities. Although there are several published practice guidelines for the treatment of EDs, and likewise, there are several published practice guidelines for the treatment of PTSD, none of them specifically address ED + PTSD. The result is a lack of integration between ED and PTSD treatment providers, which often leads to fragmented, incomplete, uncoordinated and ineffective care of severely ill patients with ED + PTSD. This situation can inadvertently promote chronicity and multimorbidity and may be particularly relevant for patients treated in higher levels of care, where prevalence rates of concurrent PTSD reach as high as 50% with many more having subthreshold PTSD. Although there has been some progress in the recognition and treatment of ED + PTSD, recommendations for treating this common comorbidity remain undeveloped, particularly when there are other co-occurring psychiatric disorders, such as mood, anxiety, dissociative, substance use, impulse control, obsessive-compulsive, attention-deficit hyperactivity, and personality disorders, all of which may also be trauma-related. In this commentary, guidelines for assessing and treating patients with ED + PTSD and related comorbidity are critically reviewed. An integrated set of principles used in treatment planning of PTSD and trauma-related disorders is recommended in the context of intensive ED therapy. These principles and strategies are borrowed from several relevant evidence-based approaches. Evidence suggests that continuing with traditional single-disorder focused, sequential treatment models that do not prioritize integrated, trauma-focused treatment approaches are short-sighted and often inadvertently perpetuate this dangerous multimorbidity. Future ED practice guidelines would do well to address concurrent illness in more depth.
精神共病在饮食失调(ED)的评估和治疗中很常见,创伤性事件和终生创伤后应激障碍(PTSD)往往是这些具有挑战性的复杂情况的主要驱动因素。鉴于创伤、PTSD和精神共病会显著影响ED的治疗结果,在ED实践指南中适当解决这些问题势在必行。一些但并非所有现有指南都提到了相关精神共病的存在,但除了参考其他疾病的独立指南外,它们大多对解决这一问题作用不大。这种脱节导致了一种“竖井效应”,即每套指南都没有解决其他共病的复杂性。虽然有几份已发表的ED治疗实践指南,同样,也有几份已发表的PTSD治疗实践指南,但它们都没有专门针对ED+PTSD。结果是ED和PTSD治疗提供者之间缺乏整合,这往往导致对患有ED+PTSD的重症患者的护理零散、不完整、不协调且无效。这种情况可能会无意中促进慢性病和多种疾病的发生,对于在更高护理水平接受治疗的患者可能尤为相关,在这些患者中,并发PTSD的患病率高达50%,更多患者患有亚阈值PTSD。尽管在认识和治疗ED+PTSD方面取得了一些进展,但针对这种常见共病的治疗建议仍未完善,特别是当存在其他同时出现的精神障碍时,如情绪、焦虑、解离、物质使用、冲动控制、强迫、注意力缺陷多动和人格障碍,所有这些也可能与创伤有关。在这篇评论中,对评估和治疗ED+PTSD及相关共病患者的指南进行了批判性审查。在强化ED治疗的背景下,推荐了一套用于PTSD和创伤相关疾病治疗计划的综合原则。这些原则和策略借鉴了几种相关的循证方法。有证据表明,继续采用传统的以单一疾病为重点的序贯治疗模式,而不优先考虑综合的、以创伤为重点的治疗方法是短视的,而且往往会无意中使这种危险的多种疾病持续存在。未来的ED实践指南最好更深入地解决并发疾病问题。