Escabi-Mendoza Jose, Diaz-Rodriguez Porfirio E, Gonzalez-Bravo Diego H, Partida-Rodriguez Eduardo
Cardiovascular Disease, Veterans Affairs (VA) Caribbean Healthcare System, San Juan, PRI.
Cureus. 2023 May 2;15(5):e38436. doi: 10.7759/cureus.38436. eCollection 2023 May.
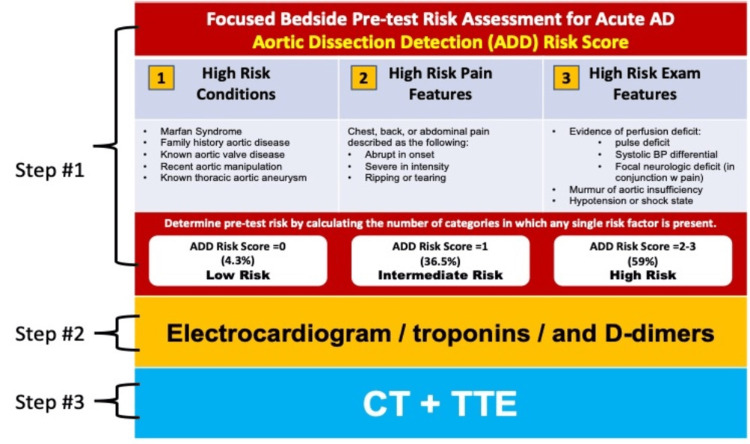
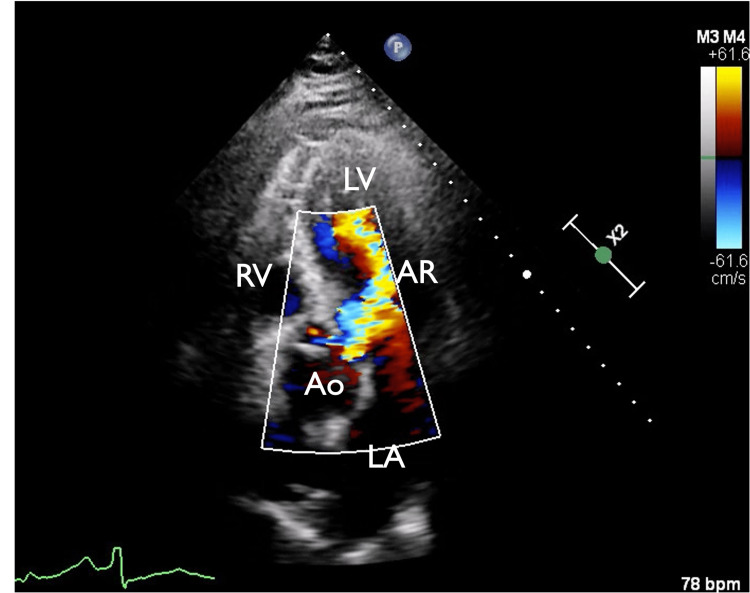
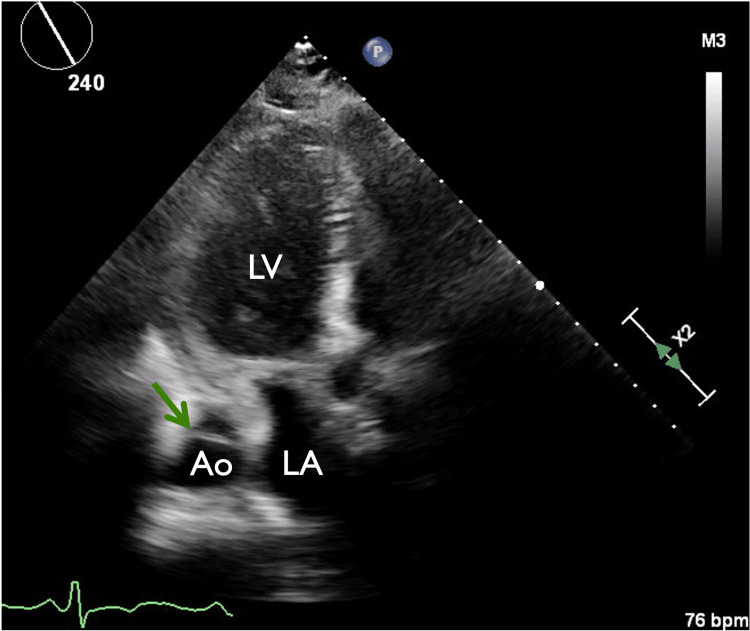
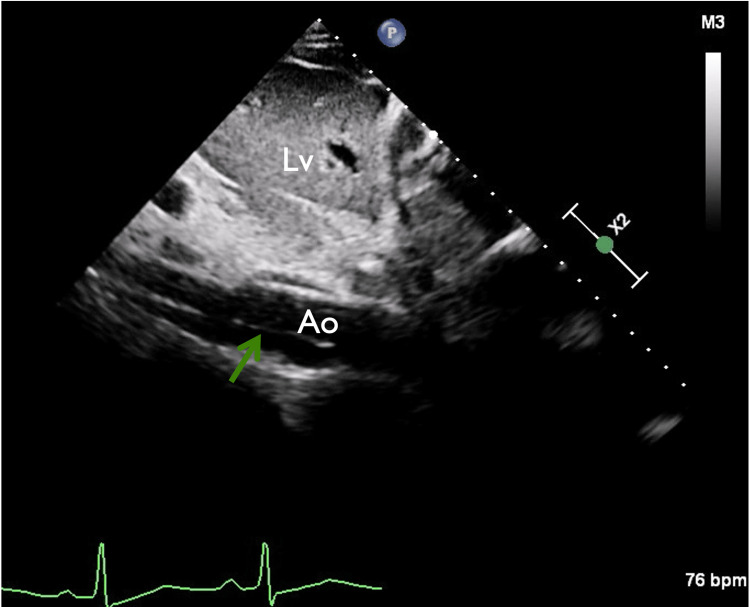
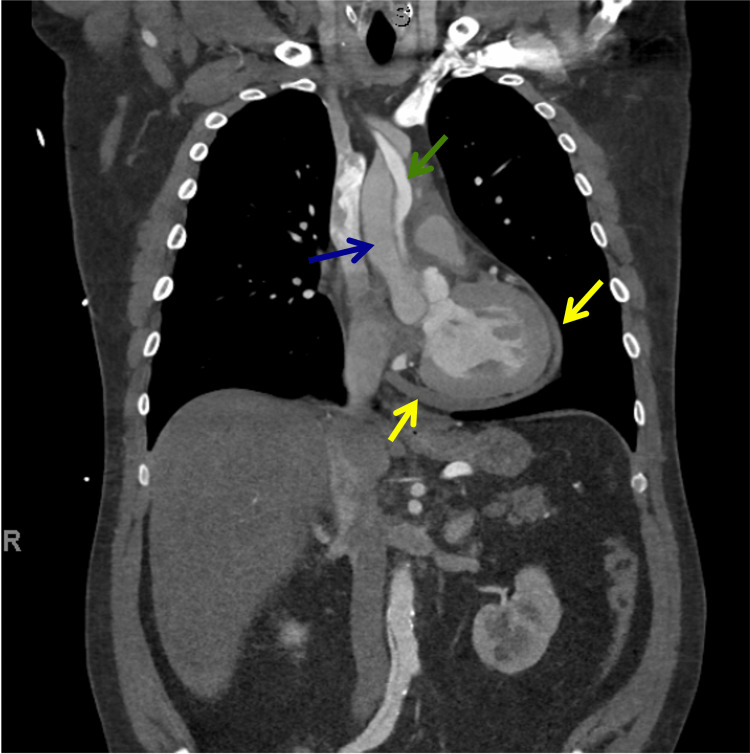
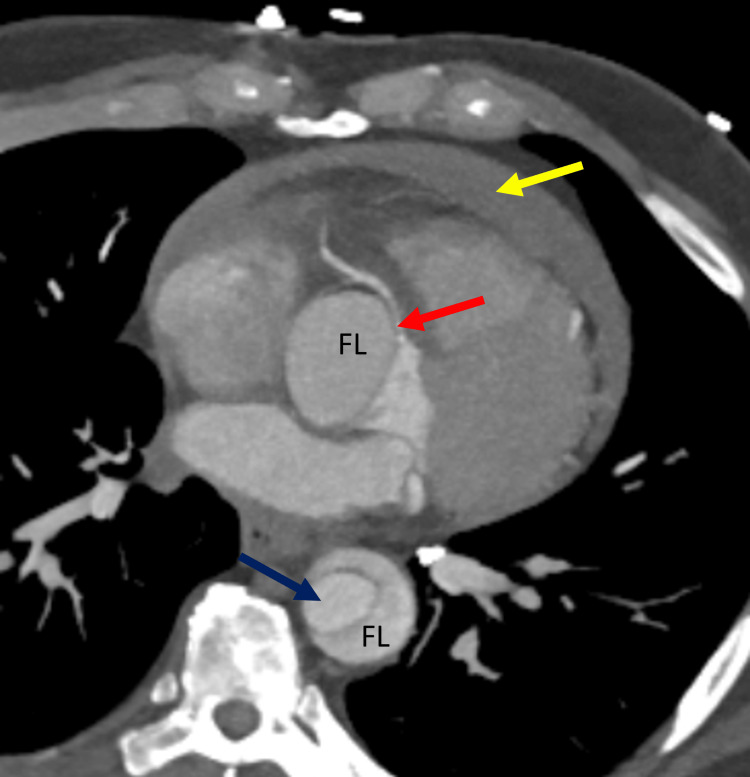
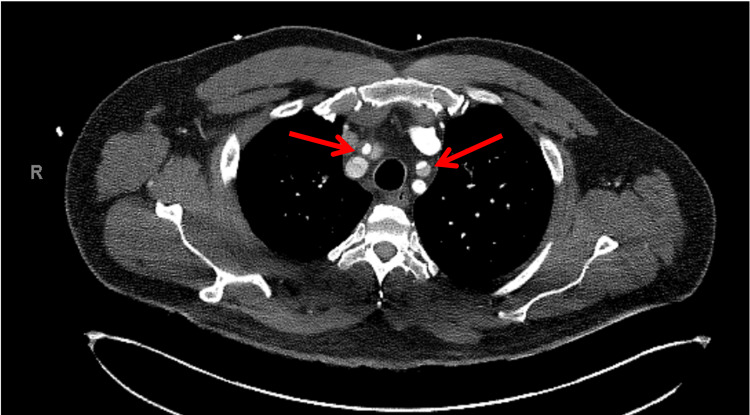
Acute aortic dissection (AD) involves the tearing of the aortic intima by shearing forces, resulting in a false lumen, which, depending on its location and extent, may lead to hemodynamic compromise, hypoperfusion of vital organs, or even rupture of the aorta. The classical presentation is a sudden chest or back pain described as sharp or ripping in quality. We present a 60-year-old male with a history of hypertension, Liddle's syndrome, obstructive sleep apnea, and chronic cannabis use for insomnia who arrived at a non-PCI hospital complaining of severe retrosternal chest pain lasting several hours in evolution that started upon masturbation. The pain was ripping in character, starting retrosternally and radiating to his neck and back. After evidence of rising troponin values, he was initially diagnosed with non-ST segment elevation myocardial infarction (NSTEMI), managed with dual antiplatelet therapy with full anticoagulation, and subsequently transferred to our institution for further care. Shortly after his arrival at our hospital, he suddenly deteriorated with recurrent chest pain and hypotension, which triggered an emergent bedside echocardiogram evaluation. This revealed a hemodynamically significant pericardial effusion, moderate to severe aortic valve regurgitation (AR), and an intimal flap visualized on the ascending and descending aorta, suggestive of an extensive AD. A computerized tomographic angiogram confirmed the diagnosis of a Stanford type A AD that required an emergent surgical pericardiotomy, ascending aorta with partial arch replacement, and aortic valve repair. Often, AD may mimic an acute coronary syndrome (ACS) or even present with an acute myocardial infarction (AMI). The appropriate diagnostic imaging evaluation prior to the initiation of anticoagulation therapy should be done in patients with higher-risk clinical criteria for AD to reduce adverse treatment outcomes. The use of a simple three-step diagnostic algorithm for acute aortic syndromes (AAS) may decrease diagnostic delays, misdiagnosis, and inappropriate therapies.
急性主动脉夹层(AD)是指主动脉内膜被剪切力撕裂,形成假腔,根据其位置和范围,可能导致血流动力学障碍、重要器官灌注不足,甚至主动脉破裂。典型表现为突发的胸痛或背痛,性质为尖锐或撕裂样。我们报告一例60岁男性,有高血压、利德尔综合征、阻塞性睡眠呼吸暂停病史,因失眠长期使用大麻,因手淫后出现持续数小时逐渐加重的严重胸骨后胸痛,就诊于一家非PCI医院。疼痛性质为撕裂样,始于胸骨后,放射至颈部和背部。肌钙蛋白值升高后,他最初被诊断为非ST段抬高型心肌梗死(NSTEMI),接受双联抗血小板治疗及充分抗凝治疗,随后转至我院进一步治疗。抵达我院后不久,他突然病情恶化,反复胸痛伴低血压,遂紧急进行床旁超声心动图评估。结果显示有血流动力学意义的心包积液、中度至重度主动脉瓣反流(AR),升主动脉和降主动脉可见内膜瓣,提示广泛AD。计算机断层血管造影证实为斯坦福A型AD,需要紧急进行外科心包切开术、升主动脉部分弓置换及主动脉瓣修复。AD常可模拟急性冠状动脉综合征(ACS),甚至表现为急性心肌梗死(AMI)。对于有AD高风险临床标准的患者,在开始抗凝治疗前应进行适当的诊断性影像学评估,以减少不良治疗后果。使用简单的三步诊断算法诊断急性主动脉综合征(AAS),可减少诊断延迟、误诊及不恰当治疗。