Eisai Inc., Alzheimer's Disease and Brain Health, Nutley, NJ 07110, USA.
Department of Neurology, Indiana University School of Medicine, Indianapolis, IN 46202, USA.
Brain. 2023 Nov 2;146(11):4414-4424. doi: 10.1093/brain/awad188.
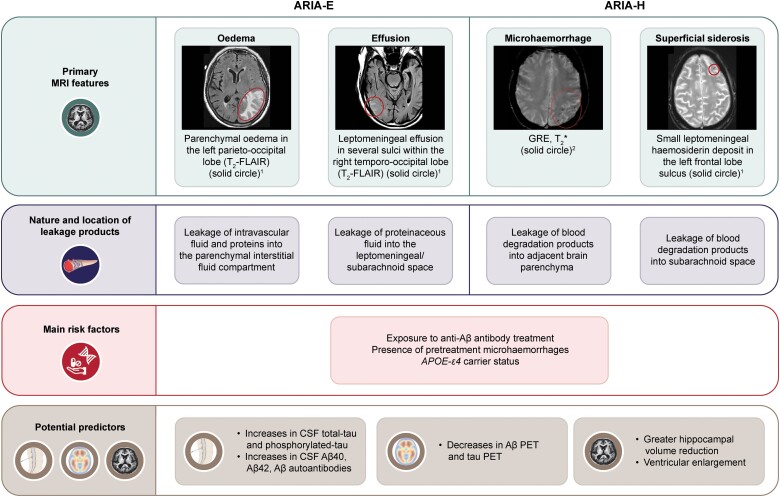
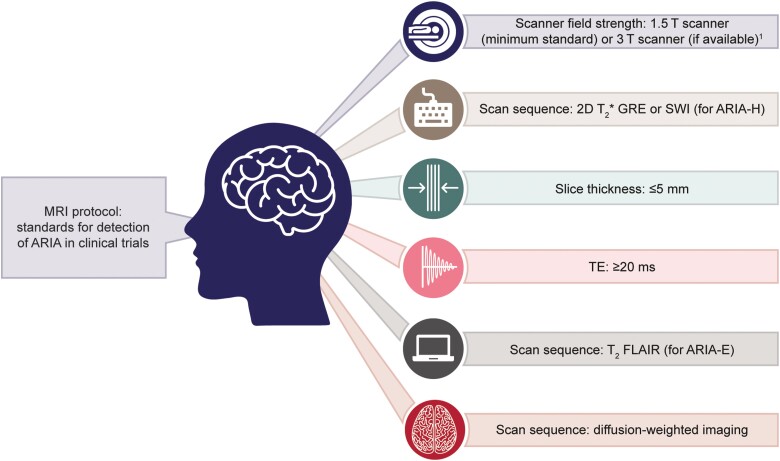
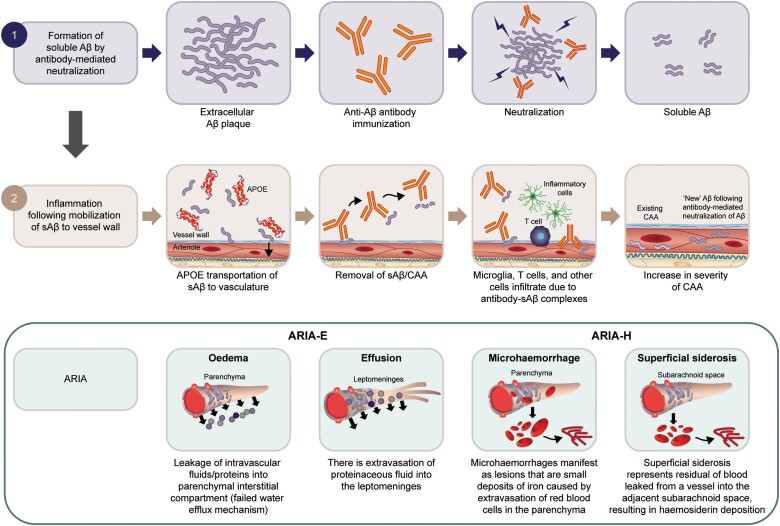
Excess accumulation and aggregation of toxic soluble and insoluble amyloid-β species in the brain are a major hallmark of Alzheimer's disease. Randomized clinical trials show reduced brain amyloid-β deposits using monoclonal antibodies that target amyloid-β and have identified MRI signal abnormalities called amyloid-related imaging abnormalities (ARIA) as possible spontaneous or treatment-related adverse events. This review provides a comprehensive state-of-the-art conceptual review of radiological features, clinical detection and classification challenges, pathophysiology, underlying biological mechanism(s) and risk factors/predictors associated with ARIA. We summarize the existing literature and current lines of evidence with ARIA-oedema/effusion (ARIA-E) and ARIA-haemosiderosis/microhaemorrhages (ARIA-H) seen across anti-amyloid clinical trials and therapeutic development. Both forms of ARIA may occur, often early, during anti-amyloid-β monoclonal antibody treatment. Across randomized controlled trials, most ARIA cases were asymptomatic. Symptomatic ARIA-E cases often occurred at higher doses and resolved within 3-4 months or upon treatment cessation. Apolipoprotein E haplotype and treatment dosage are major risk factors for ARIA-E and ARIA-H. Presence of any microhaemorrhage on baseline MRI increases the risk of ARIA. ARIA shares many clinical, biological and pathophysiological features with Alzheimer's disease and cerebral amyloid angiopathy. There is a great need to conceptually link the evident synergistic interplay associated with such underlying conditions to allow clinicians and researchers to further understand, deliberate and investigate on the combined effects of these multiple pathophysiological processes. Moreover, this review article aims to better assist clinicians in detection (either observed via symptoms or visually on MRI), management based on appropriate use recommendations, and general preparedness and awareness when ARIA are observed as well as researchers in the fundamental understanding of the various antibodies in development and their associated risks of ARIA. To facilitate ARIA detection in clinical trials and clinical practice, we recommend the implementation of standardized MRI protocols and rigorous reporting standards. With the availability of approved amyloid-β therapies in the clinic, standardized and rigorous clinical and radiological monitoring and management protocols are required to effectively detect, monitor, and manage ARIA in real-world clinical settings.
过量积累和聚集有毒可溶性和不溶性淀粉样 β 物质是阿尔茨海默病的主要标志。随机临床试验表明,使用靶向淀粉样蛋白-β 的单克隆抗体可减少脑内淀粉样蛋白-β 沉积,并确定了称为淀粉样相关成像异常 (ARIA) 的 MRI 信号异常作为可能的自发性或治疗相关不良事件。这篇综述提供了对放射学特征、临床检测和分类挑战、病理生理学、潜在生物学机制和与 ARIA 相关的风险因素/预测因素的全面、最先进的概念性综述。我们总结了现有文献和当前证据,包括抗淀粉样蛋白临床试验和治疗开发中所见的 ARIA 伴水肿/渗出 (ARIA-E) 和 ARIA 伴含铁血黄素沉着/微出血 (ARIA-H)。这两种形式的 ARIA 都可能在抗淀粉样蛋白-β 单克隆抗体治疗早期经常发生。在随机对照试验中,大多数 ARIA 病例为无症状。有症状的 ARIA-E 病例通常发生在较高剂量时,在 3-4 个月内或停药后即可缓解。载脂蛋白 E 单倍型和治疗剂量是 ARIA-E 和 ARIA-H 的主要危险因素。基线 MRI 上任何微出血的存在都会增加 ARIA 的风险。ARIA 与阿尔茨海默病和脑淀粉样血管病具有许多临床、生物学和病理生理学特征。迫切需要从概念上联系与这些潜在情况相关的明显协同作用,以使临床医生和研究人员进一步了解、考虑和研究这些多种病理生理过程的综合影响。此外,本文旨在帮助临床医生更好地检测 ARIA(通过症状或 MRI 上的视觉观察),根据适当的使用建议进行管理,并在观察到 ARIA 时做好准备和提高认识,以及帮助研究人员更好地理解正在开发的各种抗体的基本原理及其与 ARIA 相关的风险。为了促进临床试验和临床实践中的 ARIA 检测,我们建议实施标准化 MRI 方案和严格的报告标准。随着临床上已批准的淀粉样蛋白-β 治疗方法的出现,需要标准化和严格的临床和放射学监测和管理方案,以在真实世界的临床环境中有效检测、监测和管理 ARIA。