Jackson Tiara N, Sreedhara Meera, Bostic Myles, Spafford Michelle, Popat Shena, Lowe Beasley Kincaid, Jordan Julia, Ahn Roy
NORC at the University of Chicago, Chicago, Illinois, USA.
Centers for Disease Control and Prevention, Division for Heart Disease and Stroke Prevention, Atlanta, Georgia, USA.
Telemed Rep. 2023 May 15;4(1):67-86. doi: 10.1089/tmr.2023.0011. eCollection 2023.
The use of telehealth for the management and treatment of hypertension and cardiovascular disease (CVD) has increased across the United States (U.S.), especially during the COVID-19 pandemic. Telehealth has the potential to reduce barriers to accessing health care and improve clinical outcomes. However, implementation, outcomes, and health equity implications related to these strategies are not well understood. The purpose of this review was to identify how telehealth is being used by U.S. health care professionals and health systems to manage hypertension and CVD and to describe the impact these telehealth strategies have on hypertension and CVD outcomes, with a special focus on social determinants of health and health disparities.
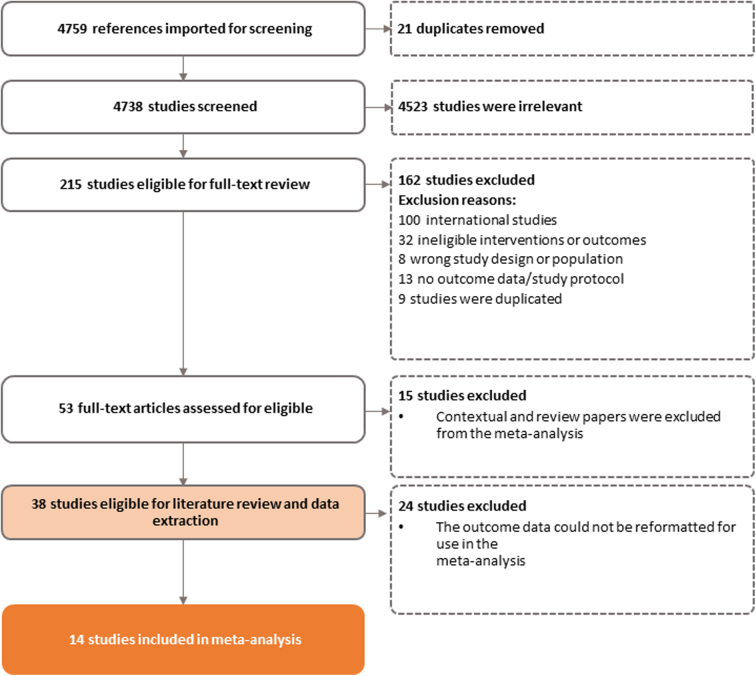
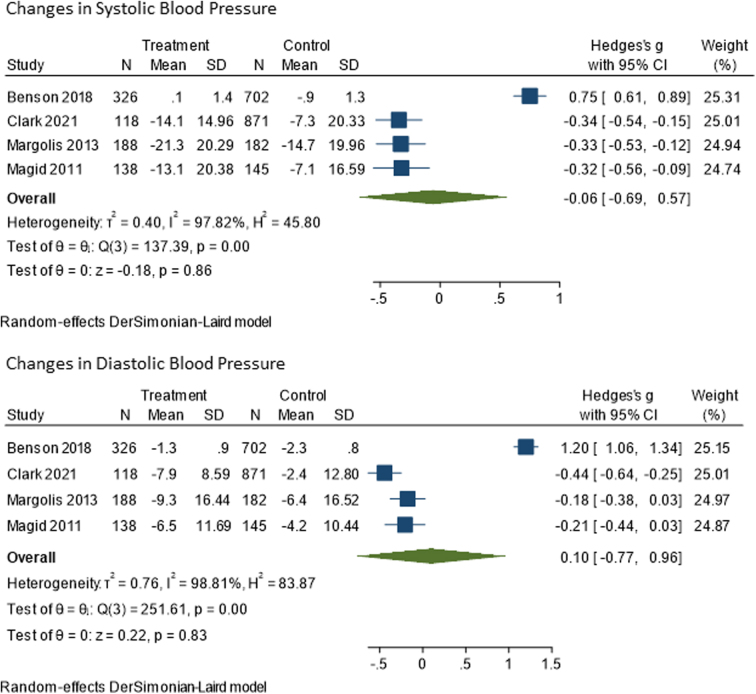
This study comprised a narrative review of the literature and meta-analyses. The meta-analyses included articles with intervention and control groups to examine the impact of telehealth interventions on changes to select patient outcomes, including systolic and diastolic blood pressure. A total of 38 U.S.-based interventions were included in the narrative review, with 14 yielding data eligible for the meta-analyses.
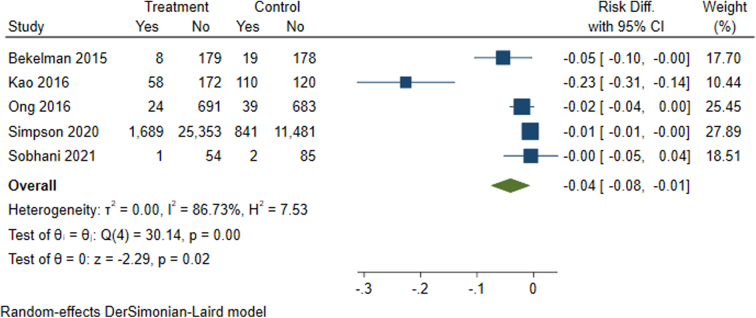
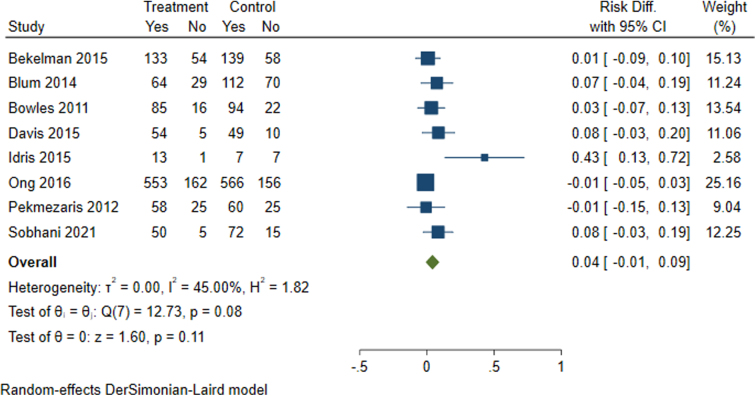
The telehealth interventions reviewed were used to treat patients with hypertension, heart failure, and stroke, with most interventions employing a team-based care approach. These interventions utilized the expertise of physicians, nurses, pharmacists, and other health care professionals to collaborate on patient decisions and provide direct care. Among the 38 interventions reviewed, 26 interventions utilized remote patient monitoring (RPM) devices mostly for blood pressure monitoring. Half the interventions used a combination of strategies (e.g., videoconferencing and RPM). Patients using telehealth saw significant improvements in clinical outcomes such as blood pressure control, which were comparable to patients receiving in-person care. In contrast, the outcomes related to hospitalizations were mixed. There were also significant decreases in all-cause mortality when compared to usual care. No study explicitly focused on addressing social determinants of health or health disparities through telehealth for hypertension or CVD.
Telehealth appears to be comparable to traditional in-person care for managing blood pressure and CVD and may be seen as a complement to existing care options for some patients. Telehealth can also support team-based care delivery and may benefit patients and health care professionals by increasing opportunities for communication, engagement, and monitoring outside a clinical setting.
在美国,远程医疗用于高血压和心血管疾病(CVD)管理与治疗的情况日益增多,尤其是在新冠疫情期间。远程医疗有潜力减少获取医疗服务的障碍并改善临床结局。然而,与这些策略相关的实施情况、结局以及对健康公平性的影响尚不清楚。本综述的目的是确定美国医疗保健专业人员和医疗系统如何利用远程医疗来管理高血压和CVD,并描述这些远程医疗策略对高血压和CVD结局的影响,特别关注健康的社会决定因素和健康差距。
本研究包括对文献的叙述性综述和荟萃分析。荟萃分析纳入了设有干预组和对照组的文章,以检验远程医疗干预对选定患者结局变化的影响,包括收缩压和舒张压。叙述性综述共纳入了38项美国的干预措施,其中14项产生了符合荟萃分析要求的数据。
所综述的远程医疗干预措施用于治疗高血压、心力衰竭和中风患者,大多数干预措施采用基于团队的护理方法。这些干预措施利用医生、护士、药剂师和其他医疗保健专业人员的专业知识,就患者决策进行协作并提供直接护理。在38项所综述的干预措施中,26项干预措施使用了远程患者监测(RPM)设备,主要用于血压监测。一半的干预措施采用了多种策略组合(如视频会议和RPM)。使用远程医疗的患者在血压控制等临床结局方面有显著改善,与接受面对面护理的患者相当。相比之下,与住院相关的结局好坏参半。与常规护理相比,全因死亡率也有显著下降。没有研究明确关注通过远程医疗解决高血压或CVD患者健康的社会决定因素或健康差距问题。
远程医疗在管理血压和CVD方面似乎与传统的面对面护理相当,对于一些患者而言,可被视为现有护理选择的补充。远程医疗还可以支持基于团队的护理提供,并可能通过增加临床环境之外的沟通、参与和监测机会,使患者和医疗保健专业人员受益。