Darst Burcu F, Shen Jiayi, Madduri Ravi K, Rodriguez Alexis A, Xiao Yukai, Sheng Xin, Saunders Edward J, Dadaev Tokhir, Brook Mark N, Hoffmann Thomas J, Muir Kenneth, Wan Peggy, Le Marchand Loic, Wilkens Lynne, Wang Ying, Schleutker Johanna, MacInnis Robert J, Cybulski Cezary, Neal David E, Nordestgaard Børge G, Nielsen Sune F, Batra Jyotsna, Clements Judith A, Grönberg Henrik, Pashayan Nora, Travis Ruth C, Park Jong Y, Albanes Demetrius, Weinstein Stephanie, Mucci Lorelei A, Hunter David J, Penney Kathryn L, Tangen Catherine M, Hamilton Robert J, Parent Marie-Élise, Stanford Janet L, Koutros Stella, Wolk Alicja, Sørensen Karina D, Blot William J, Yeboah Edward D, Mensah James E, Lu Yong-Jie, Schaid Daniel J, Thibodeau Stephen N, West Catharine M, Maier Christiane, Kibel Adam S, Cancel-Tassin Géraldine, Menegaux Florence, John Esther M, Grindedal Eli Marie, Khaw Kay-Tee, Ingles Sue A, Vega Ana, Rosenstein Barry S, Teixeira Manuel R, Kogevinas Manolis, Cannon-Albright Lisa, Huff Chad, Multigner Luc, Kaneva Radka, Leach Robin J, Brenner Hermann, Hsing Ann W, Kittles Rick A, Murphy Adam B, Logothetis Christopher J, Neuhausen Susan L, Isaacs William B, Nemesure Barbara, Hennis Anselm J, Carpten John, Pandha Hardev, De Ruyck Kim, Xu Jianfeng, Razack Azad, Teo Soo-Hwang, Newcomb Lisa F, Fowke Jay H, Neslund-Dudas Christine, Rybicki Benjamin A, Gamulin Marija, Usmani Nawaid, Claessens Frank, GagoDominguez Manuela, Castelao Jose Esteban, Townsend Paul A, Crawford Dana C, Petrovics Gyorgy, Casey Graham, Roobol Monique J, Hu Jennifer F, Berndt Sonja I, Van Den Eeden Stephen K, Easton Douglas F, Chanock Stephen J, Cook Michael B, Wiklund Fredrik, Witte John S, Eeles Rosalind A, Kote-Jarai Zsofia, Watya Stephen, Gaziano John M, Justice Amy C, Conti David V, Haiman Christopher A
Center for Genetic Epidemiology, Department of Population and Public Health Sciences, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA.
Division of Public Health Sciences, Fred Hutchinson Cancer Center, Seattle, WA, USA.
medRxiv. 2023 May 15:2023.05.12.23289860. doi: 10.1101/2023.05.12.23289860.
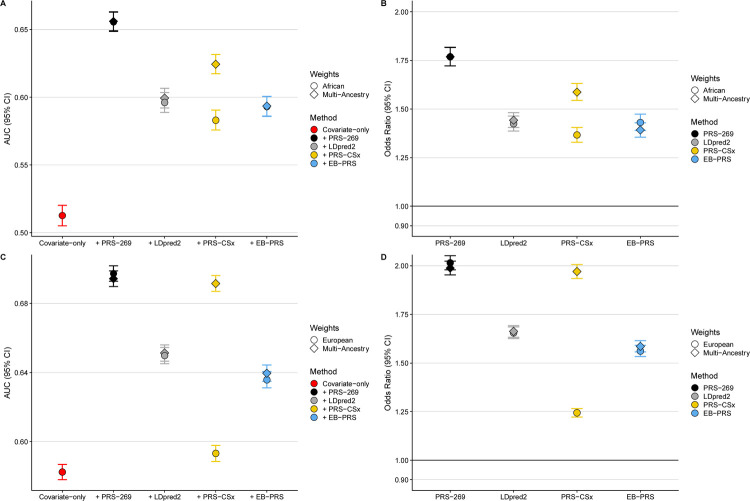
Genome-wide polygenic risk scores (GW-PRS) have been reported to have better predictive ability than PRS based on genome-wide significance thresholds across numerous traits. We compared the predictive ability of several GW-PRS approaches to a recently developed PRS of 269 established prostate cancer risk variants from multi-ancestry GWAS and fine-mapping studies (PRS ). GW-PRS models were trained using a large and diverse prostate cancer GWAS of 107,247 cases and 127,006 controls used to develop the multi-ancestry PRS . Resulting models were independently tested in 1,586 cases and 1,047 controls of African ancestry from the California/Uganda Study and 8,046 cases and 191,825 controls of European ancestry from the UK Biobank and further validated in 13,643 cases and 210,214 controls of European ancestry and 6,353 cases and 53,362 controls of African ancestry from the Million Veteran Program. In the testing data, the best performing GW-PRS approach had AUCs of 0.656 (95% CI=0.635-0.677) in African and 0.844 (95% CI=0.840-0.848) in European ancestry men and corresponding prostate cancer OR of 1.83 (95% CI=1.67-2.00) and 2.19 (95% CI=2.14-2.25), respectively, for each SD unit increase in the GW-PRS. However, compared to the GW-PRS, in African and European ancestry men, the PRS had larger or similar AUCs (AUC=0.679, 95% CI=0.659-0.700 and AUC=0.845, 95% CI=0.841-0.849, respectively) and comparable prostate cancer OR (OR=2.05, 95% CI=1.87-2.26 and OR=2.21, 95% CI=2.16-2.26, respectively). Findings were similar in the validation data. This investigation suggests that current GW-PRS approaches may not improve the ability to predict prostate cancer risk compared to the multi-ancestry PRS constructed with fine-mapping.
据报道,全基因组多基因风险评分(GW-PRS)在众多性状上比基于全基因组显著性阈值的风险评分(PRS)具有更好的预测能力。我们将几种GW-PRS方法的预测能力与最近开发的一种PRS进行了比较,该PRS基于多血统全基因组关联研究(GWAS)和精细定位研究确定的269个前列腺癌风险变异(PRS )。GW-PRS模型使用了一个包含107,247例病例和127,006例对照的大型多样化前列腺癌GWAS进行训练,该GWAS用于开发多血统PRS 。所得模型在加利福尼亚/乌干达研究中的1,586例非洲血统病例和1,047例对照以及英国生物银行中的8,046例欧洲血统病例和191,825例对照中进行了独立测试,并在百万退伍军人计划中的13,643例欧洲血统病例和210,214例对照以及6,353例非洲血统病例和53,362例对照中进一步验证。在测试数据中,表现最佳的GW-PRS方法在非洲血统男性中的曲线下面积(AUC)为0.656(95%置信区间=0.635-0.677),在欧洲血统男性中为0.844(95%置信区间=0.840-0.848),并且对于GW-PRS每增加一个标准差单位,相应的前列腺癌比值比(OR)分别为1.83(95%置信区间=1.67-2.00)和2.19(95%置信区间=2.14-2.25)。然而,与GW-PRS相比,在非洲和欧洲血统男性中,PRS 的AUC更大或相似(分别为AUC=0.679,95%置信区间=0.659-0.700和AUC=0.845,95%置信区间=0.841-0.849),前列腺癌OR相当(分别为OR=2.05,95%置信区间=1.87-2.26和OR=2.21,95%置信区间=2.16-2.26)。验证数据中的结果相似。这项调查表明,与通过精细定位构建的多血统PRS 相比,当前的GW-PRS方法可能无法提高预测前列腺癌风险的能力。