Klemann Désirée, Rijkx Maud, Mertens Helen, van Merode Frits, Klein Dorthe
Department of Gynaecology and Obstetrics, Maastricht University Medical Centre+, 6229 HX Maastricht, The Netherlands.
Care and Public Health Research Institute, Maastricht University, 6200 MD Maastricht, The Netherlands.
Healthcare (Basel). 2023 Jun 2;11(11):1636. doi: 10.3390/healthcare11111636.
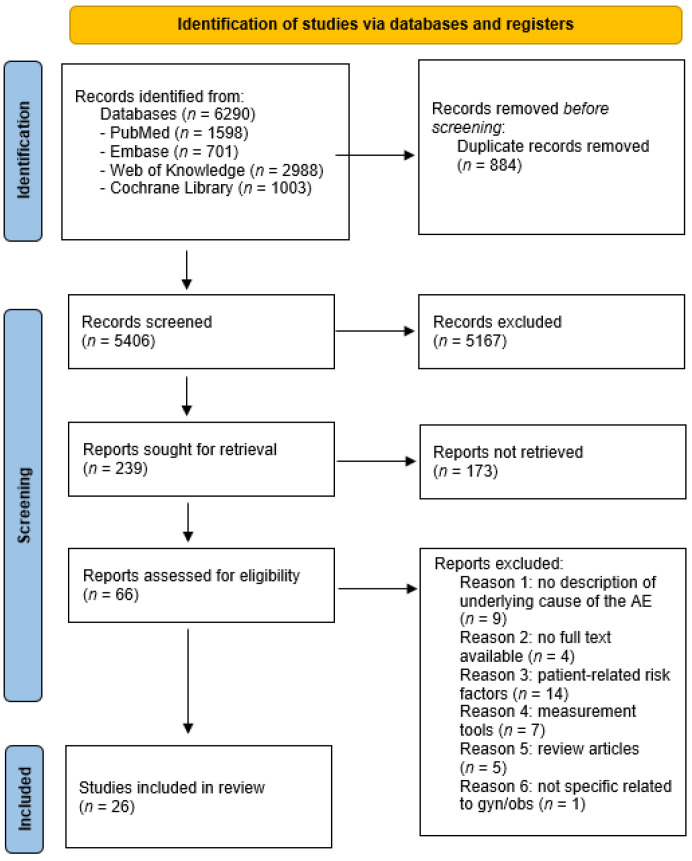
Quality strategies, interventions, and frameworks have been developed to facilitate a better understanding of healthcare systems. Reporting adverse events is one of these strategies. Gynaecology and obstetrics are one of the specialties with many adverse events. To understand the main causes of medical errors in gynaecology and obstetrics and how they could be prevented, we conducted this systematic review. This systematic review was performed in compliance with the Prisma 2020 guidelines. We searched several databases for relevant studies (Jan 2010-May 2023). Studies were included if they indicated the presence of any potential risk factor at the hospital level for medical errors or adverse events in gynaecology or obstetrics. We included 26 articles in the quantitative analysis of this review. Most of these ( = 12) are cross-sectional studies; eight are case-control studies, and six are cohort studies. One of the most frequently reported contributing factors is delay in healthcare. In addition, the availability of products and trained staff, team training, and communication are often reported to contribute to near-misses/maternal deaths. All risk factors that were found in our review imply several categories of contributing factors regarding: (1) delay of care, (2) coordination and management of care, and (3) scarcity of supply, personnel, and knowledge.
已制定质量策略、干预措施和框架,以促进对医疗保健系统的更好理解。报告不良事件就是其中一项策略。妇产科是不良事件较多的专科之一。为了解妇产科医疗差错的主要原因以及如何预防这些差错,我们进行了这项系统评价。本系统评价按照《Prisma 2020指南》进行。我们在多个数据库中检索了相关研究(2010年1月至2023年5月)。如果研究表明医院层面存在任何导致妇产科医疗差错或不良事件的潜在风险因素,则纳入研究。我们在本评价的定量分析中纳入了26篇文章。其中大部分(n = 12)是横断面研究;8篇是病例对照研究,6篇是队列研究。最常报告的促成因素之一是医疗保健延误。此外,产品和训练有素的工作人员的可获得性、团队培训和沟通也常被报告为导致险些发生的事故/孕产妇死亡的因素。我们评价中发现的所有风险因素都意味着几类促成因素,涉及:(1)护理延误,(2)护理协调与管理,以及(3)供应、人员和知识短缺。