School of Biomedical Engineering & Imaging Sciences, King's College London, St Thomas Hospital, London, SE1 7EH, UK.
School of Biomedical Engineering & Imaging Sciences, King's College London, St Thomas Hospital, London, SE1 7EH, UK.
Comput Biol Med. 2023 Aug;162:107009. doi: 10.1016/j.compbiomed.2023.107009. Epub 2023 May 16.
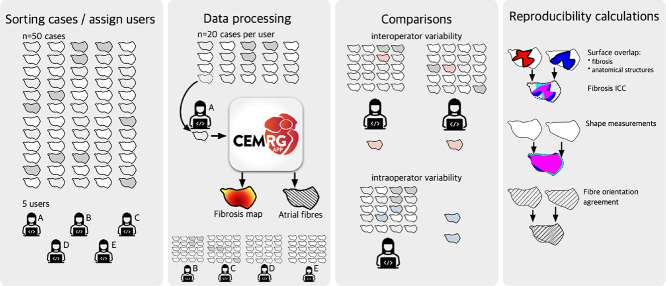
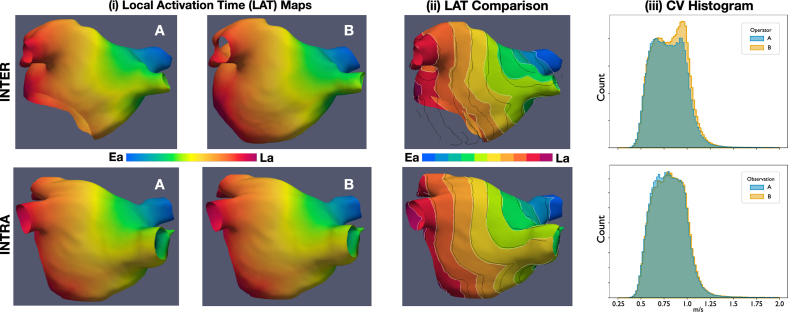
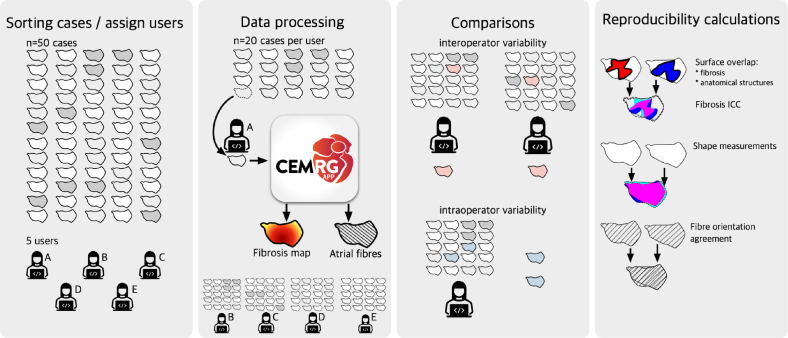
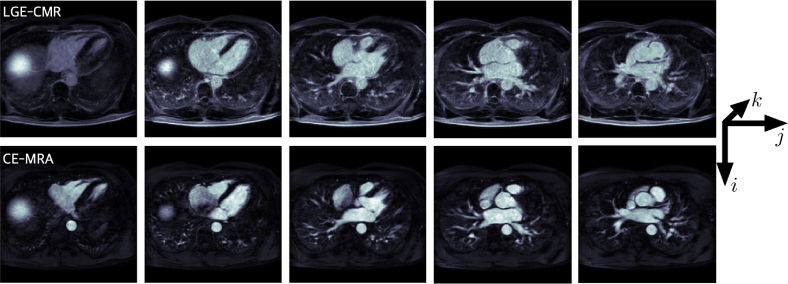
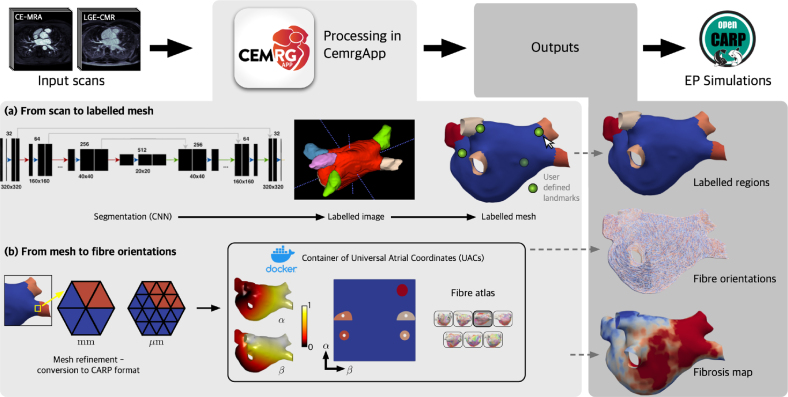
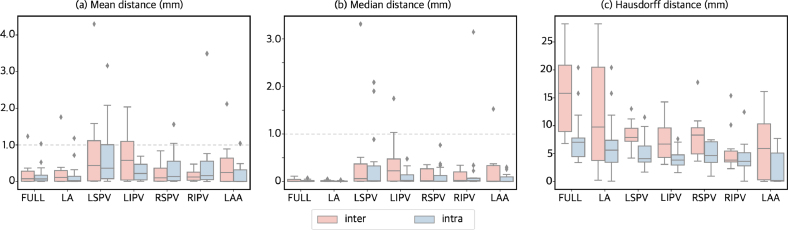
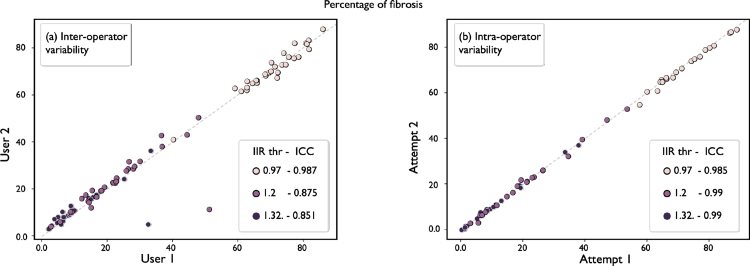
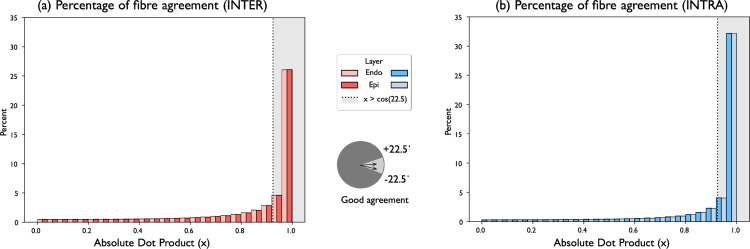
This work presents an open-source software pipeline to create patient-specific left atrial models with fibre orientations and a fibrDEFAULTosis map, suitable for electrophysiology simulations, and quantifies the intra and inter observer reproducibility of the model creation. The semi-automatic pipeline takes as input a contrast enhanced magnetic resonance angiogram, and a late gadolinium enhanced (LGE) contrast magnetic resonance (CMR). Five operators were allocated 20 cases each from a set of 50 CMR datasets to create a total of 100 models to evaluate inter and intra-operator variability. Each output model consisted of: (1) a labelled surface mesh open at the pulmonary veins and mitral valve, (2) fibre orientations mapped from a diffusion tensor MRI (DTMRI) human atlas, (3) fibrosis map extracted from the LGE-CMR scan, and (4) simulation of local activation time (LAT) and phase singularity (PS) mapping. Reproducibility in our pipeline was evaluated by comparing agreement in shape of the output meshes, fibrosis distribution in the left atrial body, and fibre orientations. Reproducibility in simulations outputs was evaluated in the LAT maps by comparing the total activation times, and the mean conduction velocity (CV). PS maps were compared with the structural similarity index measure (SSIM). The users processed in total 60 cases for inter and 40 cases for intra-operator variability. Our workflow allows a single model to be created in 16.72 ± 12.25 min. Similarity was measured with shape, percentage of fibres oriented in the same direction, and intra-class correlation coefficient (ICC) for the fibrosis calculation. Shape differed noticeably only with users' selection of the mitral valve and the length of the pulmonary veins from the ostia to the distal end; fibrosis agreement was high, with ICC of 0.909 (inter) and 0.999 (intra); fibre orientation agreement was high with 60.63% (inter) and 71.77% (intra). The LAT showed good agreement, where the median ± IQR of the absolute difference of the total activation times was 2.02 ± 2.45 ms for inter, and 1.37 ± 2.45 ms for intra. Also, the average ± sd of the mean CV difference was -0.00404 ± 0.0155 m/s for inter, and 0.0021 ± 0.0115 m/s for intra. Finally, the PS maps showed a moderately good agreement in SSIM for inter and intra, where the mean ± sd SSIM for inter and intra were 0.648 ± 0.21 and 0.608 ± 0.15, respectively. Although we found notable differences in the models, as a consequence of user input, our tests show that the uncertainty caused by both inter and intra-operator variability is comparable with uncertainty due to estimated fibres, and image resolution accuracy of segmentation tools.
这项工作提出了一个开源软件管道,用于创建具有纤维方向和 fibrDEFAULTosis 图的患者特异性左心房模型,适用于电生理模拟,并量化了模型创建的内和观察者间的可重复性。半自动管道以对比增强磁共振血管造影和晚期钆增强(LGE)对比磁共振(CMR)作为输入。五名操作员从 50 个 CMR 数据集的一组中分配了 20 个病例,总共创建了 100 个模型,以评估内和观察者间的可变性。每个输出模型包括:(1)在肺静脉和二尖瓣处开口的标记表面网格,(2)从弥散张量 MRI(DTMRI)人体图谱映射的纤维方向,(3)从 LGE-CMR 扫描中提取的纤维化图,以及(4)局部激活时间(LAT)和相位奇点(PS)映射的模拟。通过比较输出网格的形状、左心房体的纤维化分布和纤维方向的一致性来评估我们管道的可重复性。通过比较总激活时间和平均传导速度(CV)来评估模拟输出的可重复性。通过结构相似性指数测量(SSIM)比较 PS 图。用户总共处理了 60 个用于内比较和 40 个用于观察者间比较的病例。我们的工作流程允许在 16.72±12.25 分钟内创建一个模型。通过形状、以相同方向定向的纤维百分比和纤维化计算的组内相关系数(ICC)来测量相似性。仅通过用户选择二尖瓣和从瓣环到远端的肺静脉的长度,形状就有明显差异;纤维化的一致性很高,ICC 为 0.909(观察者间)和 0.999(观察者内);纤维方向的一致性很高,分别为 60.63%(观察者间)和 71.77%(观察者内)。LAT 显示出良好的一致性,其中总激活时间的绝对差异中位数±IQR 为 2.02±2.45ms 用于观察者间,1.37±2.45ms 用于观察者内。此外,平均±标准差的平均 CV 差异为 -0.00404±0.0155m/s 用于观察者间,0.0021±0.0115m/s 用于观察者内。最后,PS 图在观察者间和观察者内的 SSIM 中显示出中等良好的一致性,其中观察者间和观察者内的平均±标准差 SSIM 分别为 0.648±0.21 和 0.608±0.15。尽管我们发现模型存在明显差异,但由于用户输入,我们的测试表明,内和观察者间变异性引起的不确定性与纤维估计和分割工具的图像分辨率精度引起的不确定性相当。